Written by: Adam Tzur
Last updated: 22.01.2018
Acknowledgements: Greg Nuckols of StrongerByScience
![]()
![]()
The information presented here is not medical advice. Please consult your doctor before making lifestyle changes.

Sarcopenia
The body slowly loses its ability to build muscle mass and increase strength as we age (Horstman et al., 2012; Timmons & Gallagher, 2016; Brook et al., 2016; McLeod et al., 2016; Mitchell et al., 2016; Jang, 2016; Shad et al., 2016). This is called sarcopenia, but it has no single cause. The following is an graph from McLeod et al., 2016 and it shows muscle CSA and how it relates to age:
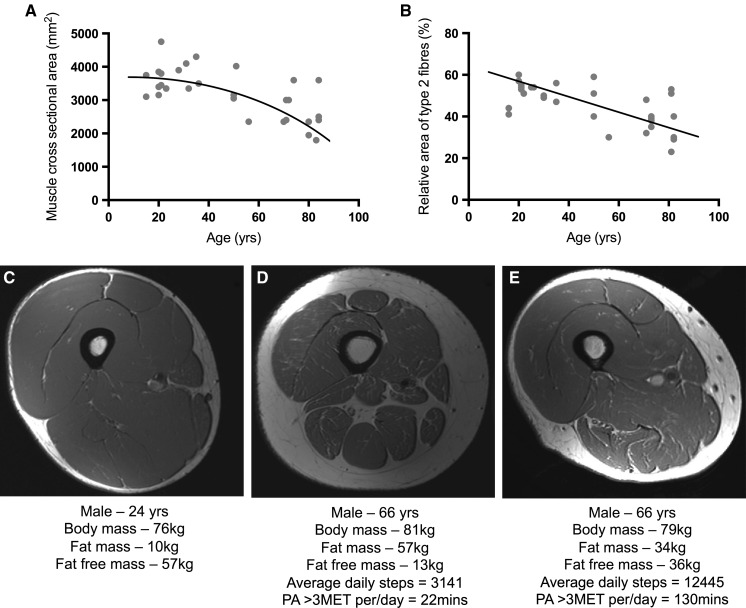
We see a clear downwards trend. In addition to this, Mitchell et al. (2012) suggest that we lose ~5% muscle mass per decade, starting somewhere in our late twenties. Tan et al. (2012) report that skeletal muscle mass drops from ~45% total body weight in our late twenties to ~27% at 70 years old. This result is pretty similar to Mitchell's. Other research groups list more dramatic numbers. They say we could lose 0.5-2% muscle mass per year, starting somewhere in our thirties/early forties 1 2 3. One study actually reports that men observed from 15-83 started atrophying after the age of 25 (McLeod et al., 2016)!!! Looking at these studies together, I think it's safe to assume that people could lose muscle mass in their thirties. However, there are notable individual exceptions (Clark and Manini, 2012), as we will see later when we discuss genetic predispositions.
In addition to muscle atrophy, we lose strength as we age. Below is an illustration from Delmonico et al., 2009. On the left graph you can see that people that lost muscle mass with aging also got much weaker. On the right side, the subjects gained muscle mass, but still lost strength.

So researchers now believe that there are other mechanisms that impact strength beyond muscle mass. These mechanisms become downregulated with age so that even if you maintain or increase muscle mass, you're bound to get weaker (Mitchell et al., 2012; Clark and Manini, 2012; Wagatsuma and Sakuma, 2014). Several research teams estimate that we lose ~2-4% strength per year as we get older 4 5 6. Note: this number may not directly apply to you if you're actively doing strength training. We will discuss this in more detail further down.
Researchers now think sarcopenia comes from a combination of many factors, like: muscle disuse, neuron atrophy, CNS inefficiency, declining anabolic hormones, low protein intakes, anabolic resistance, micronutrient deficiency, genetic predisposition, diseases, mitochondrial inefficiency, decreasing muscle quality, and chronic inflammation. I'm going to discuss these mechanisms in the following section.
What causes muscle loss?
Inactivity, atrophy, and muscle quality
As we get older, we're much more likely to be sedentary. Many researchers wonder whether we become sedentary before we lose muscle mass, or whether we become sedentary because we lose muscle mass 7 (Peterson and Gordon, 2011). It's hard to say for sure, but some researchers think muscle mass decreases because muscles lose their quality. By quality I mean ability to produce force. For example, muscles generate less force per unit of CSA with age (Mitchell et al., 2012; McGregor et al., 2014). More fat is deposited into muscle tissue possibly making muscles more inefficient (McGregor et al., 2014; Delmonico et al., 2009; Wagatsuma and Sakuma, 2014). Looking at molecular mechanisms, some studies suggest aging muscles develop problems with muscular contractions because of an impaired calcium release mechanism 8.
Anabolic resistance
Similarly to muscle quality, anabolic resistance is also a local mechanism. When we look at how the body responds to exercise, we see that it adapts by making our muscles more resistant to change. This has been studied in young lifters and it's called anabolic blunting (Coffey et al., 2005; Mangine et al., 2015; Gonzalez, 2015; Gonzalez et al., 2015a; Noguiera et al., 2015). In short, this blunting means that muscle protein synthesis and mTOR become harder to activate the more trained you get. In theory, this would partially explain why we experience diminishing returns as we grow bigger and stronger. So how does this link to aging? There’s now a debate whether anabolic resistance could happen to older people as well, even if they’re untrained. Some studies find that older lifters show anabolic resistance to strength training and nutrition (Kumar et al., 2009; Vingren et al., 2010; Horstman et al., 2012; Markofski et al., 2015; Moore et al., 2015; Wall et al., 2015; Moro et al., 2016; Timmons & Gallagher, 2016; Loenneke et al., 2016; McLeod et al., 2016; Mitchell et al., 2016; Shad et al., 2016). The theory is that the body slowly downregulates MPS and mTOR in a response to aging.
On the other hand, a new systematic review has just been published and it finds only partial support for the claim that MPS signalling becomes weaker with age (Shad et al., 2016). Shad et al. think a big reason there’s so much contradiction in the MPS literature is because of methodological differences between studies. A big limitation to Shad's review is that the majority of the studies they included only measured mixed muscle protein synthesis. This type of MPS does not predict hypertrophy. We need to look at myofibrillar protein synthesis (myoMPS) (Moore et al., 2009) if we want a shot at predicting gains (and in many cases, myoMPS does not predict gains either) (ASM). Here's an illustration of the differences between mixed MPS and myoMPS post-exercise: (illustration from Damas et al., 2015).
Ideally, Shad et al. would discard studies that measured mixed MPS and only analyze myoMPS. And since Shad isn't here right now I'll do it myself; out of the 24 studies included in Shad's review, 5 dealt with myoMPS. Three studies found a clear difference between young and old in terms of myoMPS responses (Babraj et al., 2005; Cuthbertson et al., 2005; Kumar et al. 2012), one study found differences at some time-points (Kumar et al. 2009), while one study found no difference (Atherton et al., 2016).
Here's an illustration of the differences, as per Kumar et al., 2009:
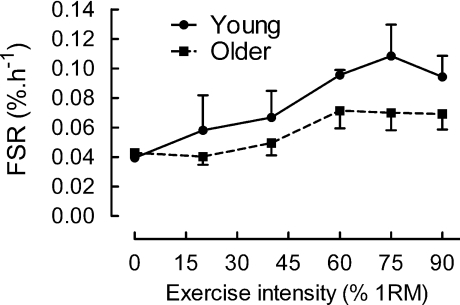
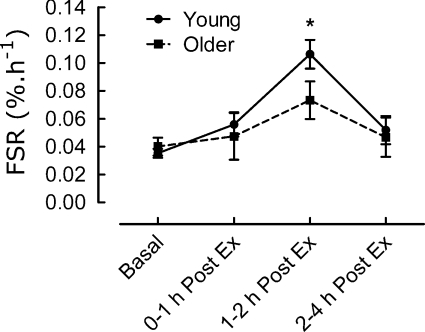
When we eliminate the mixed MPS studies, we see greater support for the anabolic resistance theory. There are also other studies outside of Shad et al's. review that support this (Welle et al., 1993; Welle et al., 1995; Yang et al., 2012). Several of these studies show that mixed MPS is actually quite similar between old and young, but myoMPS is blunted in the old 9 10.
You might come across studies entitled "Aging does not impair the anabolic response to a protein-rich meal" (Symons et al., 2007), and they might seem convincing at first sight, but once you read conclusions like "Mixed-muscle FSR increased by approximately 51% in both [old and young]" you get disappointed at the researchers for not controlling for myofibrillar MPS.
From the information I've presented here, I think it's likely that MPS-related anabolic resistance exists. Beyond the studies that I've explicitly linked in this section, many of the studies and reviews I discuss in this article agree that MPS-related anabolic resistance is real. However, I will add the limitation that I have not systematically reviewed the literature, so it is possible that there are studies out there that contradict this hypothesis. In that sense, my conclusions are tentative, pending further evidence (as is everything in science...). Furthermore, do note that MPS correlates with gains only in some situations. In most situations researchers have looked at to date, it does not (ASM).
Declining anabolic hormones
Beyond mechanisms that affect the muscle tissue locally, the body experiences systemic changes with age. Most notably, systemic anabolic hormones like IGF-1, GH, and testosterone are reduced (Ryall et al., 2008; Vingren et al., 2010; Horstman et al., 2012; Tan et al., 2012; Fan et al., 2016; Budui et al., 2015). These reductions probably leads to muscle loss (Horstman et al., 2012; Mouser et al., 2016; Vitale et al., 2016). Testosterone drops by about 1-3% per year, beginning sometime during your thirties 11 12, GH and IGF-1 secretion declines by 14% per decade after the age of 30 13, and tissues become more insulin insensitive (Vitale et al., 2016)
Here's a relevant illustration by Ryall et al., 2008:

Inflammation
As we age, our bodies develop constant low-level inflammation (Jensen, 2008; Peterson and Gordon, 2011; Fan et al., 2016). Chronic inflammation likely affects muscle mass and strength negatively 14 15 16 17 18 19 20. There are several causes (Fan et al., 2016):

It gets even worse if you have diabetes, because this condition is characterized by inflammation (Park et al., 2009; Kalyani et al., 2014; Khor et al., 2014; Koster and Schaap, 2015; Jang, 2016; Vitale et al., 2016).
Nervous system inefficiency and neural activation
The nervous system degenerates with age and it goes through multiple changes. Notably, the PNS loses muscle neurons (Frontera et al., 2011; Clark and Manini, 2012; Tintignac et al., 2015). These neurons are nerve cells that go from the spine to muscles and they control muscle contraction. Many authors now think this loss of neurons partially explain why muscles atrophy and we become weaker as we age (Kwan, 2013; McLeod et al., 2016) 21 22 23. However, others say that this might be the case, but we should wait for stronger evidence before we conclude anything for sure 24 (Manini et al., 2013). On the other hand, Manini's review is from 2013, and newer reviews think there is enough evidence to make conclusions (Sakuma et al., 2015). Beyond the physical decrease in motor neurons, the nervous system generally becomes more inefficient at sending messages. Manini et al. (2013) describe this as "neural noise" (i.e. static noise) which leads to "breakdown in communication between brain and muscle". Aging people could therefore have problems with voluntary neural activation and lowered maximal contraction 25.
From Clark and Manini, 2012: (Dynapenia = "Dynapenia is the age-associated loss of muscle strength that is not caused by neurologic or muscular diseases")

Genetics
Genetics is a huge and complicated subject so I will try to simplify as much as possible here. Researchers think people have different phenotypes. A phenotype is basically a collection of observable traits (physical features, mental abilities, etc.). Phenotypes are created from an organism's genes and their interaction with the environment. We now think that some phenotypes are at greater risk for sarcopenia because of heritability. It's estimated that muscle strength is 30-85% genetically inherited, while muscle mass is 45-90% inherited (Roth, 2012; Pereira et al., 2013), but the estimations vary depending on which review and study we look at (Tan et al., 2012). Update: a new systematic review and meta-analysis suggests strength is about 50% inherited (Zempo et al., 2016).
In addition to heritability, we have individual variation. Some individuals could lose a lot of muscle mass as they age, while others do not (Clark and Manini, 2012; Tan et al., 2012). This has been studied recently, and some older people that do strength training actually lose muscle mass. These people are referred to as non-responders, and it also happens in young subjects. You can see the non-responders at the bottom of this graph by Churchward-Venne et al., 2015:

There are some issues with measuring fat mass, LBM, water, etc. using DXA/BIA and similar methods. However, I won't go into that topic in this review.
We can also look at individual genes and analyse their relationship to muscle loss. The ACE, ACTN3, MSTN (myostatin), CNTF and VDR (vitamin D) genes are promising 26 (Khor et al., 2014). Some authors claim each of these genes can contribute 1-3% when it comes to skeletal muscle variation 27. It's possible that genes can also have synergistic effects. For example some genes could have a much stronger effect when combined 27. In that sense, no gene exists in isolation.
Low protein intakes
It's highly likely that sarcopenia is affected by low protein intakes (Shad et al., 2016). In fact, we need more protein the older we get (Moore et al., 2015; Philips, 2015; Shad et al., 2016; Mitchell et al., 2016; McLeod et al., 2016; Loenneke et al., 2016; Courtney-Martin et al., 2016; Baum et al., 2016). Adults that eat a lot of protein maintain ~40 % more muscle mass compared to those that eat very little protein 28.
Micronutrient deficiency
Micronutrients are vitamins and minerals. It generally goes without saying that it's really important to get enough micros regardless of age. There are some micros that are particularly interesting; vitamin D. In general, low vitamin D levels could lead to muscle atrophy and reduced strength (Robinson et al., 2012; Roth, 2012; Wagatsuma and Sakuma, 2014; Khor et al., 2014; Wakabayashi and Sakuma, 2014; Budui et al., 2015). Nevertheless, there's a big BUT here: pretty much every review of the vitamin D literature agrees that results are inconclusive, so we can't say for sure how much vitamin D deficiency matters when it comes to strength and muscle mass.
Other causes
I don't have the time nor inclination to look at every single potential cause for sarcopenia in this article, but I will link you an illustration from (Miljkovic et al., 2015) that summarizes some potential causes:
