![]()
![]()

What You Will Learn
Understand why some people adhere to the ketogenic diet, and why some people fail.
What We Did and Why
We systematically searched the ketogenic literature for studies on adherence. We gathered data on carb intake, calorie intake, ketone levels and how many people dropped out from their diet.
Our goal is to determine if people can stick to the ketogenic diet in the long-term.
In What Scenarios Do People Adhere to the Ketogenic Diet?
In scientific studies, there are 3 common scenarios where people adhere well to the diet:
- Highly motivated people (e.g., elite athletes)
- Studies where food is provided for the participants.
- People in metabolic wards (e.g., hospitals) where the researchers closely monitor the participants. They can only eat the food they are given. This is forced adherence and does not reflect real-life adherence.
(Read more: At what ketone level are people in ketosis?).
How Long Do People Adhere to the Ketogenic Diet?
People who are left to their own devices generally do not adhere well to the diet. They typically start strong, but have a hard time adhering to the diet after 1-3 months. Carb intake increases and ketone levels drop. In particular, overweight people and diabetics struggle with adherence.
Sign up to the Newsletter for More Nutrition Articles
[newsletter]
Is It Easier or Harder to Adhere to Keto vs. Other Diets?
We started by analyzing dropouts: how many people drop out of keto groups versus control diet groups?
The odds of dropping out were similar for all diets. About 24% of people drop out regardless of diet (Odds Ratio = 1.05, P = 0.66). (Jump to our meta-analysis of 30 keto studies.) 2We also wanted to compare self-reported food intake vs. the control diets, but this data is not accurate enough for statistical analysis. The reason is that people often underreport how much they eat
In conclusion we do not yet know whether ketogenic diets are easier or harder to adhere to compared to other diets. We do know that people struggle adhering to all diets over time. Some people do very well on some diets, yet we don’t know why.
The practical takeaway is that you should try different diets, and see which one suits you best. A high protein diet is always a good choice if your goals include fat loss, muscle gain, and/or better satiety.
Hopefully, future research will give us better tools to predict dietary adherence.
“ … no diet has yet been shown to be uniformly easier to stick with than another in the long run.” - Freedhoff and Hall, 2016
Video summary by PictureFit
Summary Infographic
Adherence to a diet is crucial (Johnston et al., 2014; Freedhoff and Hall, 2016; Bray and Siri-Tarino, 2016). An objective way to measure ketogenic adherence is via ketone levels (Nymo et al., 2017; Cipryan et al., 2018). If ketones increase, we know that the person is restricting carbohydrates. If ketone levels fall, then participants are probably not adhering to the diet.
Studies with normal weight, diabetic, or obese participants
After doing a systematic search of the ketogenic literature, we identified ten suitable studies (read more about our inclusion and exclusion criteria). You can see data from these ten studies in the line chart below.
Eight groups never reached ketosis above 0.5 mmol/l. Four were in borderline ketosis (0.3–0.49 mmol/L BHB) by the end of the study. Only two groups were clearly in ketosis at one point during the study.
An interesting trend is that ketone levels decrease over time.
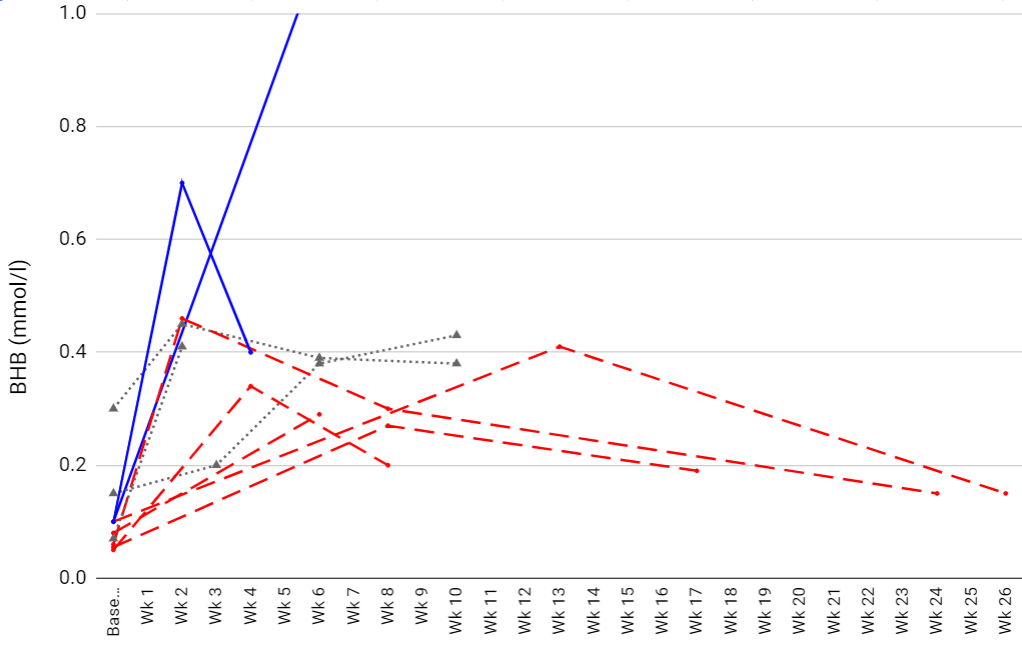
Figure: every line represents a group of people who were aiming to achieve ketosis in various studies. The solid blue lines were in ketosis at least once during the study. Dotted grey lines were in borderline ketosis. Dotted red lines were not in ketosis at the end of the studies. We chose studies that reported BHB levels in the blood. Every line represents one keto group from a study. Note that every study aimed for a carb level that would lead to ketosis (≤70 g per day).
These data suggest that people, primarily diabetics and the obese, struggle to adhere to the ketogenic diet.
Note: some of our reviewers have pointed out that decreasing BHB levels are expected, because they are an adaptation to the diet. They are not an indication of poor adherence. This observation is currently anecdotal and we could not find any published data on this adaptation.
Though, it should also be said that most keto scientists use ketone levels as an objective marker of adherence (see scientific quotes below). Sci-Fit is currently writing an article on this topic.
| Study | Ketone level at the end of the fat loss period (BHB mmol/L) |
| Krebs | Week 13
2.28 |
| Gibas and Gibas | Week 10
0.43 |
| Noakes | Week 8
0.2 |
| Brehm 2003 | Week 26
0.15 |
| Brehm 2005 | Week 17
0.19 |
| Fleming | Week 6
0.29 |
| Meckling | Week 10
0.38 |
| Brinkworth (B) | Week 8
0.3 |
| Cipryan | Week 4
0.4 |
| Keogh | Week 2
0.41 |
Studies in elite athletes, metabolic wards, and with close follow-up
There are also several studies that had tight control over what the participants ate. We didn’t include these in the primary analysis because they do not tell us anything about real-life adherence (external validity).
In other words, we can’t tell if people can adhere to a diet if they are being fed pre-planned meals in a hospital while being monitored. Yet, these tightly controlled studies are very useful if we want to figure out mechanisms related to ketosis (internal validity). For example, if we wanted to test how the ketogenic diet affects energy expenditure, we would prefer to do it in a metabolic ward.
In these types of studies, people have much higher BHB levels:
- Johnstone et al., 2008 (metabolic ward): 1.52 mmol/L urinary BHB at week 4
- Hall et al., 2016 (metabolic ward): 0.76 mmol/L BHB over 4 weeks
- Goday et al., 2016 (feeding study): 1 mmol/L BHB at week 4
- Johnston et al., 2006 (feeding study): 0.72 mmol/L BHB at week 2
- Gomez-Arbelaez et al., 2018 (feeding study): 1 mmol/L BHB at C-2 (week 5.6)
- Burke et al., 2017 (elite athletes): 1.8 mmol/L BHB at week 3
- Wilson et al., 2017 (close follow-up): 0.85–1.4 mmol/L BHB at weeks 4–10
Here are ketone graphs from two of these studies:

Figure: Hall et al., 2016. Ketones remain elevated in a metabolic ward
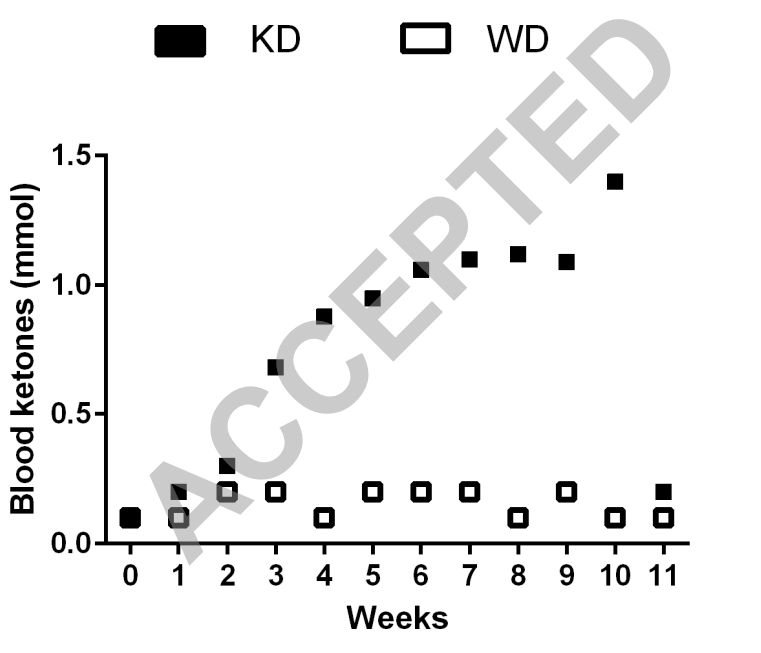 Figure: Wilson et al., 2017. Ketones remain elevated for two months before refeeding carbohydrates. Note, this is not a metabolic ward study.
Figure: Wilson et al., 2017. Ketones remain elevated for two months before refeeding carbohydrates. Note, this is not a metabolic ward study.
The metabolic ward studies show us that ketones can stay elevated when participants are “forced” to adhere to the diet. This is contrasted with the free living studies where participants’ BHB levels typically drop over time. The difference seems to be adherence.
If there is an adaptation that decreases BHB levels over time, it has not shown itself in these studies. At the very least, we must reflect on why BHB levels are consistently higher in metabolic wards, feeding studies, and studies with motivated athletes.
We have created two line charts of the studies. The first shows us how many carbohydrates people ate over time. The second looks at short-term studies.
Note that the data is-self reported carbohydrate intake. People often tend to say they ate less than what they really did. This is called underreporting (Baranowsky et al., 1986; Schoeller, 1990; Drougas et al., 1992; Lichtman et al., 1992; Fries et al., 1995; Buhl et al., 1995; Schoeller, 1995; Heitmann and Lissner, 1996; Scagliusi et al., 2003; Okubo et al., 2008; Scagliusi et al., 2008; Bartholome et al., 2013; Capling et al., 2017). Hence, people most likely ate more carbs than what they reported.
Long-term studies
The data in the graph below suggest that very few keto groups are able to eat less than 50 grams of carbohydrates over time. In most studies, they revert to a higher non-ketogenic carbohydrate intake.
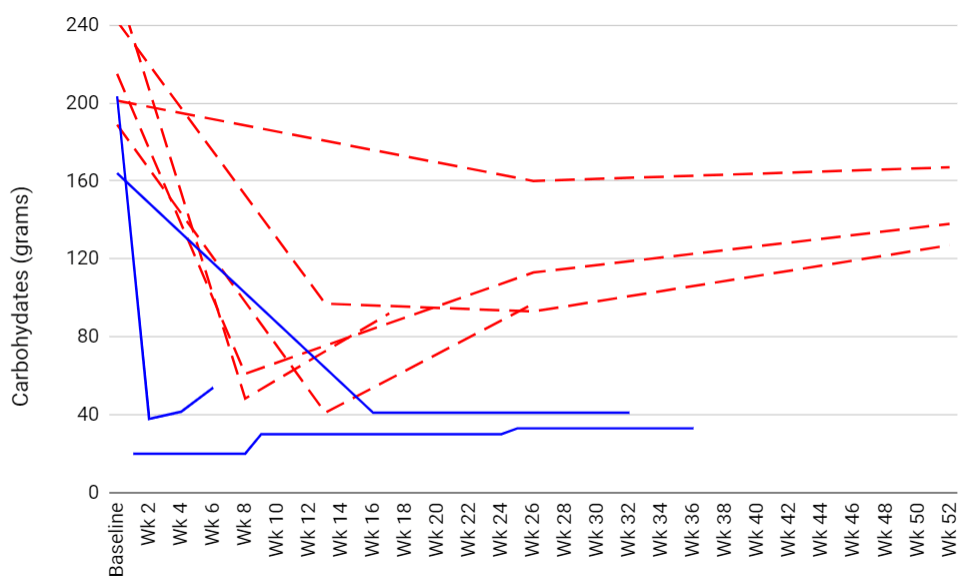
Figure: every line represents a group of people who were aiming to eat less than 70 grams of carbs. The solid blue lines report adhering to the diet. Dotted red lines were not adhering to their diet by the end of the study. This graph only includes studies that tracked how carb intake changed over time3Studies with 2+ time point measures after baseline.
Short-term studies
For studies shorter than 13 weeks, people report that they adhere to the diet.

Figure: every line represents a group of people who were aiming to eat less than 70 grams of carbs. The solid blue lines report adhering to the diet. Dotted red lines were not adhering to their diet. We only included short-term studies with single time point measures in this graph.
Odds ratio meta-analysis
If we pool the numbers, the included ketogenic diet studies had a total of 1307 participants, of which 319 (24.4%) dropped out from the studies. The control diets had a total of 1294 participants, of which 311 (24%) dropped out.
Meta-analysis OR = 1.05, P = 0.66.

Forest plot: Every line/row represents dropouts from one study. The red dots represent the odds ratio which could favor either the keto or control groups. If the red dot is to the right of the vertical line, then the participants in the keto group had higher odds of dropping out. And vice versa. The horizontal lines represent the 95% confidence interval. Wide lines represent greater uncertainty. Note that more participants increase certainty while few participants decrease certainty.
Odds ratio sensitivity analysis
If we remove the studies with zero dropouts, there is no change to the outcome:
