Written by: Adam Tzur
Acknowledgements: Brandon Roberts
Article length: ~3200 words
Last updated: 25.04.2018
Studies reviewed: 60+
![]()
![]()

Can You Build Muscle in a Calorie Deficit?
Discover whether you can build muscle in a calorie deficit. Learn about the role of protein, strength training, and proper rest.
Deficit gaining, recomping, or bulking?
We are similar, yet different
Athletes have different levels of success when bulking, as shown in the graph below. The same is true for cutting (Garthe et al., 2011). Not everyone can gain muscle and lose fat at the same time. It might depend on factors like:
- Age
- Gender
- Training level (Helms et al., 2014b),
- How steep the caloric deficit is (Helms et al., 2014a; Robinson et al., 2015; MacKenzie-Shalders et al., 2016)
- Your protein intake (citations further up)
- Diet and training program adherence
- Body fat. Low body fat increases your risk of losing muscle mass (van der Ploeg et al., 2001; Rossow et al., 2013; Kistler et al., 2014; Murphy et al., 2014; Robinson et al., 2015; Huovinen et al., 2015; Hulmi et al., 2016).
- How much and which type of cardio you do (i.e. interference effect) (Helms et al., 2014b)
- How close you are to your genetic potential

Garthe et al., 2012 - Athletes respond differently to bulking.
A great deal of studies show that there are high-responders, low-responders, and non-responders to training. This means that our bodies react differently to similar training programs and diets. I won’t go into details here, but check out my article on it, and Greg’s, as well.
Cutting with little body fat
You might be more likely to lose muscle mass if you cut calories when your body fat is already low (i.e. below 7-10% for men) (Rossow et al., 2013; Helms et al., 2014a; Kistler et al., 2014; Huovinen et al., 2015; Robinson et al., 2015). In two studies on women bodybuilding competitors, they lost fat and muscle mass during contest prep but it was probably because they hit 12% body fat by the end (van der Ploeg et al., 2001; Hulmi et al., 2016). This is very low for women! To illustrate it, women suffering from anorexia nervosa have 9-13% body fat (Mayo-Smith, 1989; Mayer et al., 2005). The menstrual cycle can stop when body fat becomes very low (Halliday et al., 2016). Some suggest 12% for women is akin to 4% for men. Here’s a comparison image from Builtlean:

I don’t want to encourage you to drop to unhealthy bodyfat levels that are akin to eating disorders. So please consider your level of body fat before you decide to restrict calories. Drastic calorie reductions might lead to disordered eating (Manore et al., 2015). Although, this shouldn’t be a problem for most of us since we’re more likely to have too much body fat rather than too little.
What is the best method to gain muscle and lose fat?
Preface
“The best method” depends on your diet and program (Helms et al., 2014b). As we see in the graph below, some women were able to gain lean mass, but most did not (though they did go to very low body fat levels, which affects gains!). They all used their own diets and training programs.

Figure by Hulmi et al., 2016
With that caveat out of the way, let’s see what the research has to say.
Bulking
Bulking (eating in a surplus) is the traditional way of gaining muscle mass. You can gain slowly (lean bulk) or quickly (dirty bulk). It’s sometimes said that a dirty bulk is better for putting on muscle mass, but you will also gain a lot of fat at the same time (Garthe et al., 2012). In the figure below, the dirty bulk group gained a lot more fat than the lean bulk group.
“The excess energy intake in a weight gain protocol should (...) be considered carefully since greater rates of gain are likely to include larger increases in body fat storage in already strength-trained athletes” - Garthe et al., 2012

Bar chart by Garthe et al., 2012 (Edited for clarity) - The white group (NCG) ate ~3600kcal, black group ate ~3000kcal
Some have pointed out that the amount of energy you consume affects how much muscle you can build:
“a significant correlation between total energy intake and gains in lean mass (r = .43, p = .04) was demonstrated” - MacKenzie-Shalders et al., 2016
Others support this idea as well, the more energy and protein you consume, the more gains. From a metabolic ward study:

Figure by Bray et al., 2012 - Note that the participants were in a metabolic ward and they did not strength train during the intervention and still gained LBM. High and medium protein groups increased their energy expenditure by about 200 kcal by the end of the study
Though if you don’t consume enough protein, the extra energy is stored as fat, as you can see in the low-protein group (same study):
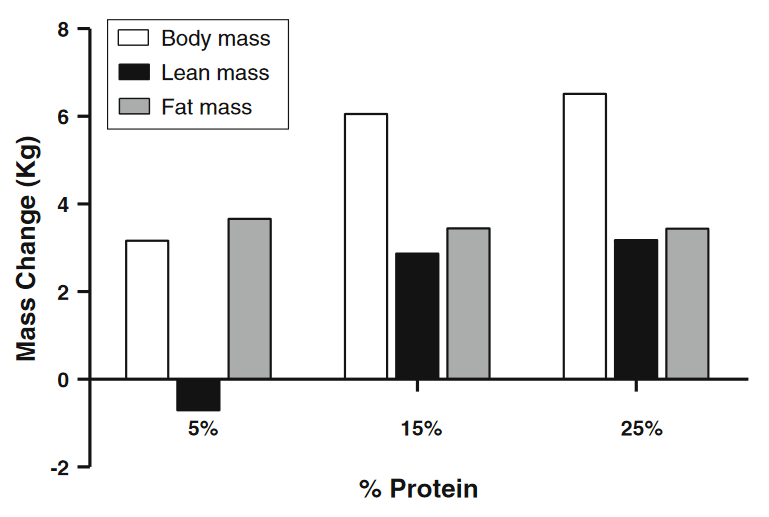
Bar chart by Churchward-Venne et al., 2013, based on Bray et al., 2012. This shows us that it’s necessary to consume enough protein if we want to gain LBM.
"With the low protein diet, more than 90% of the extra energy was stored as fat. Because there was no change in lean body mass" - Bray et al., 2012
In conclusion for bulking, there's some evidence that more calories might lead to greater LBM gains, but the evidence isn't very strong and we need more studies.
Gaining in a caloric deficit
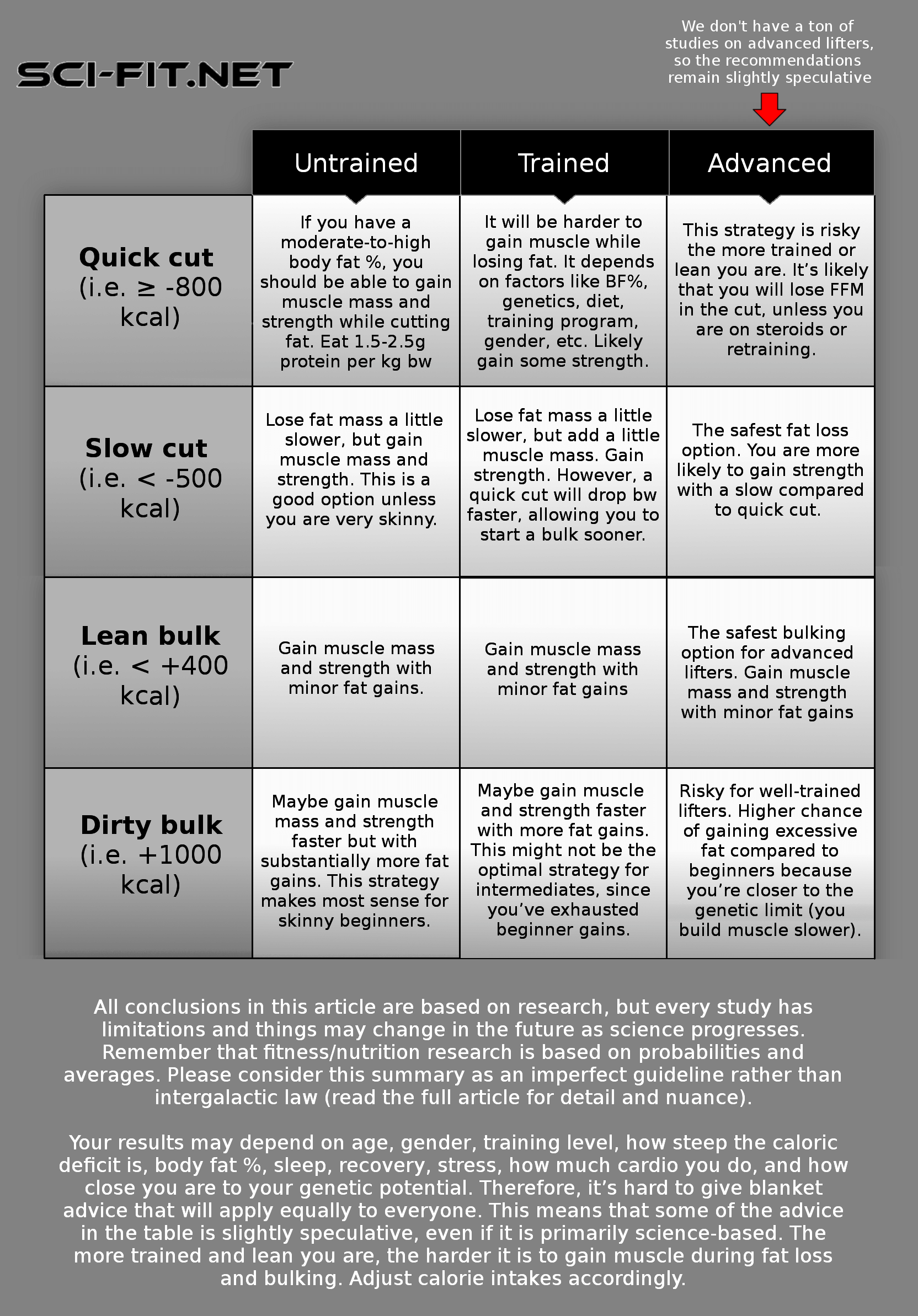
It is possible to gain muscle mass and strength in a caloric deficit, but there are many factors that decide whether it will work for you or not. It’s probably a good idea to go for deficit gaining if you’re overweight, or a beginner/novice. If you’re both, even better.
If you are, however, a lean athlete with years of strength training experience, it might work, it might not. I can’t speak in certainties. You could try it, just make sure to keep protein high (i.e. 2g per kg bw), go for a slow cut (maximum -500kcal per day), get enough sleep & recovery, avoid excessive stress, have the right genetics, and use a solid strength training program. The better your body composition is, the harder deficit gaining will be for you, in all likelihood (Helms et al., 2014b; Rossow et al., 2013; Kistler et al., 2014; Huovinen et al., 2015). The graph below shows that endurance athletes with lower body fat %, lost FFM on a cut. Those with body fat over 10% did not.

Correlation by Huovinen et al., 2015. Note that they didn’t follow a strength training program in this study and that the sample size was small.
Gaining strength is easier, because more studies suggest that you can gain strength even if you’re quite well trained (see the study overview table above for details).

Bar chart by Garthe et al., 2011 - Novice/intermediate lifters gain more strength on the BP during a slow cut (SR) compared to a quick cut (FR).