![]()

5 Overtraining Myths Explained by Science
Do you think overtraining is real? In this article, we explore the scientific data behind 5 overtraining myths.
Overtraining prevalence and duration
Many studies have looked at the prevalence of OT. According to some studies, OT could affect anywhere between 7% to 20% athletes per season [1-3, 121], or 7% to 31% per year, in collegiate athletes [5-6, 42]. The number is probably higher in elite athletes [2, 7]. For example, a study of elite British athletes report that 15-35% males and 4-15% females became overtrained during a season [8]. Six out of 15 interviewed US Olympic athletes reported symptoms of overtraining 90 days before the 1996 and 1998 Summer Olympics [9].
In summary, if we include athletes of all levels, the prevalence of OT is anywhere from 4% to 35% per season. 30% to 65% of athletes will become overtrained at least once in their career [1, 8]. Athletes that were diagnosed with overtraining once, were almost guaranteed (91%) to become diagnosed again [1]. But, the stats depend on factors such as the gender, workload, competitive level, and sport of the athlete [8]. Once diagnosed, OT can last anywhere from a couple of months to several years [10], with some cases lasting up to 7 years [11].
These data show overtraining is a real challenge for athletes of all levels and we should not ignore risk factors and early signs. Furthermore, we should focus on prevention because OT might reappear several times during an athlete’s career.
With that said, we can’t exclude the possibility that some of these athletes were simply overreaching, so the prevalence stats might be inflated [1]. We will go into more detail regarding the distinction between overtraining and overreaching later.
Consequences of overtraining

What are the consequences of becoming overreached and/or overtrained? Generally speaking, overtraining affects several systems in the body. It could, arguably, lead to:
- Acute and chronic immunosuppression [1, 12-14, 74]
- Mental health issues: depression, anxiety, and lowered libido [1, 2, 12-16]
- Decreased performance [1, 5, 12, 14, 17, 30]
- Weight loss [2, 12]
- Sleep problems [1, 2, 5, 14, 19-20, 26, 34, 82, 176]
- Higher risk of injury [16, 17, 21, 22] which is also linked to improper periodisation and overuse [23]
- Fatigue [1, 3-5, 12, 14, 15, 18, 24-22, 176, 177]
- Increased risk of illness [12, 27]
- Slow strength and endurance gains [28, 29]
However, as Meeusen et al., 2013 note, many of these signs of overtraining aren’t necessarily symptoms that can be used to diagnose an athlete. This is because many of the symptoms are similar between non-functional overreaching and overtraining. In addition, there is inter-individual variation when it comes to symptoms of overtraining [30]. With that said, if an athlete is feeling depressed, frequently sick, underperforming, losing weight, has sleep problems and feels fatigued, then there’s probably some issue that needs to be looked into. Writing it off as overreaching or ignoring it might be risky.
How to prevent overtraining

Preventing overtraining from a mental aspect
During the past 30 years, more and more research has focused on the mental aspect of athletic performance. From many investigations, it’s quite clear that performance affects and is affected by emotional states [3, 33]. Whenever training load is drastically increased, our mood may degrade [1, 33-34], and when mood is worsened, performance drops [3]. Hence, mood and performance have a complex and perhaps symbiotic relationship.
Elite athletes have completely different mood profiles compared to the average population. This is called the “iceberg profile” [3]. As seen in the illustration below, these athletes score lower than the population average on negative moods, while they score much higher on feelings of vigour. But these mental benefits aren’t restricted to elite athletes, they also apply to active individuals [3].
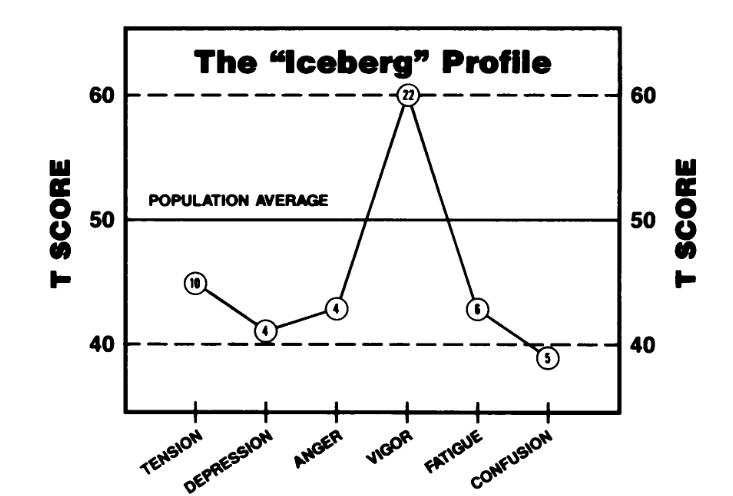
The iceberg profile by Morgan et al., 1987
Mindset (expectation vs. reality)
It’s common for top athletes or aspiring athletes to have high expectations and the ability to push themselves, which allows them to perform at a high level. The issue with this resilience is that if combined with unrealistic expectations and perfectionism, it could lead the athlete to push himself or herself to the point of overtraining [11, 18, 36-39]. Several research groups have now found associations between athletes’ feelings of self-worth and their sports performance. They now think that a perfectionistic drive to improve self-worth via sports is one of the ways athletes develop overtraining [38-41]. Some athletes end up giving up their sport completely because of this pressure [39, 40].
Recent research now suggests both external perfectionism (expectations of others) and internal perfectionism (what you expect of yourself) both increase risk of burnout and giving up sports [40], as shown in the graph below. External expectations of perfection were much more likely to make the athlete feel burned out [185] and quit their sport [40].
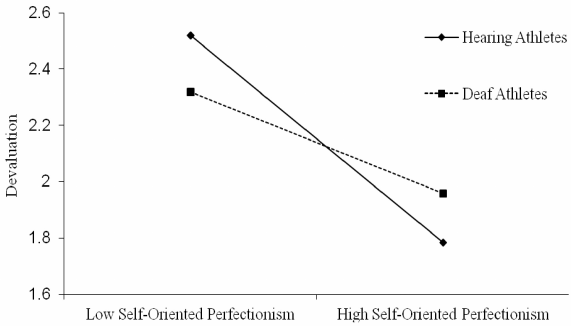
Graph by Ho et al., 2015
If we were to apply this to our own lives, a good place to start would be your thoughts, expectations, and mindset. Do you need to win at all cost? Do you find yourself never satisfied? Do you think more is always better? Is your self-esteem tied up with your training goals and training performance? Are expectations from family, friends, and coaches stressing you out? If you answer yes to some of these, it’s possible that you might eventually be at risk for UPS. We’re not saying ambition and motivation are bad things, but at some point excessive and unrealistic expectations could be preventing progress, even if that sounds counter-intuitive.
Below we suggest some more science-based “prehab” overtraining prevention strategies that should safeguard you from developing UPS.
Minimizing mental stress
Intuitively, it might seem unlikely that mental stress could lead to UPS. Even so, a lot of studies and reviews now suggest mental stress is a risk factors for burnout [3, 5, 30, 42, 47]. There are different explanations for why this might be.
Mental stress could:
- Slow post-exercise recovery [43, 44]
- Slow gains in performance, hypertrophy, and endurance [3, 28, 29]
- Cause some active individuals to train even more [44]
Morgan et al. developed a mental health model which predicts performance:
"This mental health model assumes that positive mental health is associated with high performance levels, whereas mood disturbances are predicted to result in performance decrements. Predictions based upon this model have been found to have an accuracy of approximately 80% in a series of studies"
(Morgan et al., 1987)
This means that stressful situations like a breakup, death of a family member or close friend, or inter-personal conflicts could be triggers for lowered performance [28, 29] and possibly UPS. However, it is unlikely that mental stress would cause overtraining by itself. The model does imply mental health and performance are not separated factors, but rather intertwined and interdependent [1, 3, 16, 28, 29, 33] For example, it’s hard to perform at your best if you’re depressed.
There are several ways to approach this challenge. First of all, it would be prudent to keep a mental-health diary. The most commonly used “mental diary” is the Profile of Moods (POMS) questionnaire which you can download here. It allows you to compare your mental state on a weekly or monthly basis, depending how often you take it. Changes in your mental health score could predict development of UPS. Below is a bar chart that compared healthy POMS scores to overtraining scores (OTS = overtraining syndrome).

Bar chart by Meeusen et al., 2013 (Adapted from Raglin & Morgan, 1994)
To destress, we have some obvious solutions, like spending more time with friends and family while limiting time spent on stressful activities like training or competition. Indeed, social support reduces burnout risk [46, 47].
A lot of research is now being done in alternative ways to lower stress levels. Recently, researchers have examined mind-body therapies and how they affect mental stress.
Mind-body therapies (meditation, relaxation techniques, yoga)
Mind-body therapies could:
- Reduce mental stress and improve mood [11, 48, 50-54, 184]
- Improve immune function [45, 55-58]
- Improve sleep [59-61]
- Reduce inflammation [62]
All of the factors mentioned above are linked to UPS. In addition to these benefits, there’s reason and evidence that mindfulness and mind-body therapies may prevent the development of overtraining [63].

Illustration: Moen et al., 2015 (edited by us for clarity)
As you can see in this illustration, mindfulness was positively associated with sport and school achievement, and negatively associated with stress and burnout. At the same time, stress was positively associated with burnout, and negatively associated with both school and sport achievement. In some studies, subjects who were mentally stressed gained less strength and endurance compared to low-stress subjects [28, 29]. Practically speaking, it would be a good idea to start doing meditation or some sort of MBT when you feel you’re overreaching, feeling stressed out, or generally at risk for developing UPS.
The importance of social support and relationship with coach
Lu et al., dropped a very interesting study in 2016 about how an athlete's relationship with their coach is integral to their motivation [47]. They found that life stress was linked with burnout and so was poor support from the coach. When life stress was low, athletes who had poor support and little mental resilience were much more likely to feel burned out compared to athletes who were resilient and/or had better social support. But the magnitude changed when life stress was high, at which point most athletes felt burned out (5 times as many symptoms, compared to baseline). The athletes that were least likely to experience burnout had high mental resilience and solid support from their coach.
Check the graphs below for details:
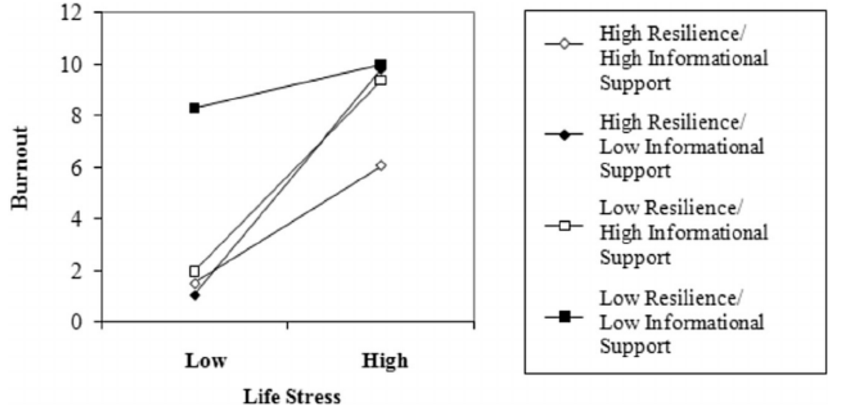
Lu et al., 2016 - Figure 1: The relationship between informational support from coach and personal resilience

Lu et al., 2016 - Figure 2: The relationship between social support from coach and personal resilience
Other studies also affirm the importance of a good coach-athlete relationship when it comes to burnout [64].
If we condense the social research in the psychology sections of this guide, it is important to have a supportive coach that has realistic expectations for you and doesn’t force you to train more than you are capable of. The coach should help buffer the stress you feel going through life, and not add to it. Based on the evidence, a bad coach could make you feel burned out and possibly develop UPS.
Proper training programming and periodisation
Improper periodization (excessive exercise combined with under-recovery) is one of the primary reasons athletes underperform [30]. Yet, athletes in sports with low physical demands can still develop overtraining [30], so it’s possible to underperform due to non-training-related stressors [1, 5, 11, 18, 30, 176].
Researchers now recommend us to utilize proper periodisation to prevent overtraining [10, 66, 183]. It’s beyond the scope of this review to explain programming and periodisation theory, but there are some practical principles we can follow to minimize risk of excessive training:
- Keep a training log which includes Rate of Perceived Exertion (how difficult every exercise/drill felt), bodyweight, workout duration and intensity, volume (for resistance training), and any pains or aches [1, 10, 26, 183]. We recommend combining this training log with the mental health log described in the previous section.
- Planned deloads: Follow a training program that has built-in periods of increasing total workload (overreaching) followed by periods of relatively lowered total workload. Deloads do not have to be complete absence from exercise or training.
- Reactive deloads: If the athlete feels symptoms of UPS, like worsened mood and excessive fatigue, it would be pertinent to reactively deload. Especially if these negative changes are accompanied by increased training stressors and non-training-related stressors.
- Personalized periodization [1]: Changes should be made to the program if it’s too hard or too easy. This could be done by manipulating weekly volume, intensity, duration, and frequency in response to how the athlete feels and performs. Some athletes may respond well to high volumes with low training frequencies, while others might respond better to high intensities. Personalization requires the coach and athlete to accept the notion that more isn’t always better.
How long can you train hard?
“4 weeks is considered the maximum time that athletes can withstand intensification of already high training loads”
(MacKinnon, 2000)
We also want to warn about training too hard in a single session. A potentially life-threatening condition called Exertional Rhabdomyolysis could develop [67-72, 178-179]. Worst case scenario, this condition could lead to kidney failure [69, 72, 73]. For example, one Norwegian man was hospitalized with Rhabdomyolysis after a bout of crossfit where he was tasked to do 45 overhead squats followed by 90 pullups, no breaks. Obviously, this condition only occurs in extreme circumstances, but athletes should be aware of the possibility nonetheless.
Recovering from exercise
A consensus statement from the European College of Sport Science and the American College of Sports Medicine recommends at least one rest day per week to prevent overtraining [1].
As we’ve mentioned previously, mental stress could impact recovery. There are some researchers that have specific recommendations for this:
"Stress, (...) moderated the recovery trajectories of muscular function and somatic sensations in a 96-hour period after strenuous resistance exercise. Therefore, under conditions of inordinate stress, individuals may need to be more mindful about observing an appropriate length of recovery."
(Stults-Kolehmainen et al., 2014)
Illnesses, infections, and diseases
It would also be a good idea to temporarily stop training or reduce workload in the case of illnesses, infections, diseases, or injuries [1, 12, 26, 74]. It’s hard to give specific recommendations on this because these problems can vary in their duration and how debilitating they are. But as a general rule of thumb, pushing yourself when you are sick or injured, is not a good idea yet moderate exercise is okay when the symptoms are mild [1, 12, 26, 27]. Researchers speculate this happens due to immunosuppression and/or altered immune function.
Furthermore, excessive alcohol drinking can impair recovery, reduce immune function, and should be avoided if maximal performance is the goal [27, 75-78]. However, light drinking is probably safe [76]. Just be careful not to drink excessively up to 72 hours after intense exercise, when immune function may be temporarily decreased. This is called the open window theory [74] and its duration may be altered by recovery and exercise:
“With insufficient rest there can be a cumulative effect of consecutive days of intensive training (i.e. the “window” staying open for a longer period of time)”
(Hackney and Koltun, 2012)
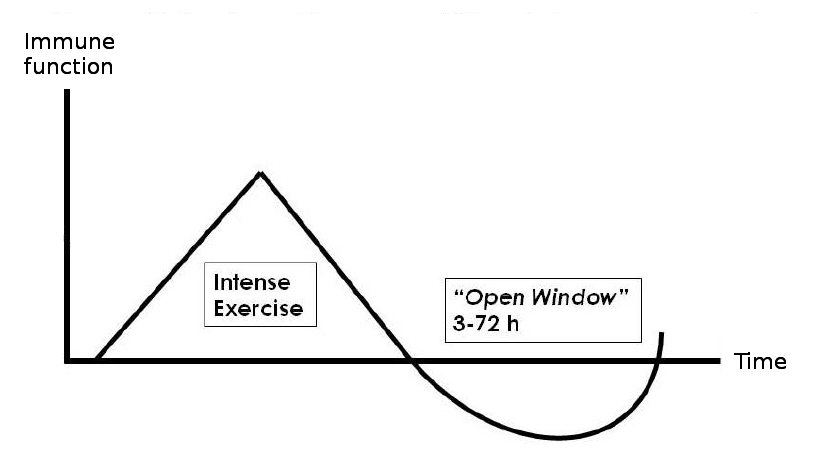
Graph based on materials from Hackney, 2013
Some research groups think the data on the open window is limited and causal links between exercise, immunosuppression, and infection risk haven’t been fully established yet [1, 79, 80]. A recent review explains some interesting new developments in sports immunology; like some athletes may have a genetic predisposition for upper respiratory illness. The suggested explanation is that the athletes have a stronger inflammatory response to exercise, which could affect immunity [81]. This makes us speculate: Is there a genetic basis for UPS? Are some individuals predisposed to UPS?
Sleep
As individuals overreach and underperform, they might experience sleep issues [2, 5, 14, 18, 19, 34, 82] but sleep issues might also lead to burnout [1, 26]. Hence sleep problems might be one of the causes and effects of UPS.
Research shows sleep is important for the immune system and chronic sleep loss can predispose athletes to sickness [83]. Prolonged periods of disturbed sleep can reduce cognitive ability, worsen mood state and slow motor skill acquisition – all of which affect performance [20, 176]. Tying into the hormonal section of this review, some of these disturbances could be responsible for sleep disturbances [84].
As mentioned previously, meditation and reduced workload could alleviate sleep issues [59-61]. Given that sleep is so important for recovery [20, 85, 86], it would be best to get adequate sleep on a frequent basis [10, 20, 85]. Some authors suggest at least 7-9 hours per night to maintain athletic performance [20, 85]. Sleep deprivation and getting less than 6-7 hours of sleep per night is associated with impaired immune and cognitive function, slow recovery, impaired glycogen repletion, worsened mental health (including depression), pain, and a host of various diseases and illnesses [20, 85-92]. Getting more than 9 hours of sleep per night might be a good idea if you are recovering from illness or injury [85, 92].
Some researchers note that there’s not enough evidence that performance becomes worse with short-term sleep loss and they would like to see more evidence before they can provide objective sleep recommendations [93, 94].
Nutrition
There are numerous opinions on how nutrition affects overtraining. Some focus on how important high carbohydrate and fluid intake is to prevent glycogen depletion and dehydration [1]. While others recommend a sliding scale of carb intake that is closely matched to the predicted energy expenditure of athletes [95].
Protein is also critical, with inadequate protein intake reported in some chronically fatigued athletes [96]. In fact, endurance athletes who increase their daily protein intake to 3g/kg during a period of overreaching have better performance and less of a stress response to training [97]. Other research shows 1.7g/kg/day is not sufficient to improve performance and recovery [98].
In respect to resistance training, supplementing with amino acids may help preserve performance and alleviate muscle soreness (DOMS) [99]. Moreover, high protein diets can reduce the risk of upper respiratory tract infection during high intensity training [97].
There’s no perfect diet to prevent overtraining [100, 101]. However, chronic glycogen depletion could lead to overtraining [102-104]. Low muscle glycogen can impair performance because of inadequate fuel for training [105]. Furthermore, a lack of fruit and vegetables can also lead to slower rates of muscle regeneration [8]. It can also impair sleep, which increases the risk of overtraining [100]. However, one study of swimmers who consumed low carbohydrates experience more fatigue but do not reach the threshold needed to have overtraining [106].
A simple way to avoid low glycogen levels is to avoid low carb and keto diets. Training with low glycogen levels may increase inflammatory cytokines, which contributes to overtraining [107]. Meal timing may matter as well because glycogen resynthesis is elevated post-exercise. Practically speaking, we could eat carbs and protein after exercise to maximize resynthesis between training sessions [108-110, 186]. This is probably more important for athletes who train multiple times per day.
Many athletes travel, which can make proper nutrition more difficult. This can in turn contribute to risk of overtraining by creating inadequate protein, carbohydrate or total energy intake. We know proper nutritional intake is important, so it’s no surprise that avoiding nutritional deficiencies should be part of preventing UPS. The literature also leans toward a higher carbohydrate and protein intake for athletes to enhance performance and recovery.
Energy Balance
Caloric restriction, insufficient carbohydrate and/or protein intake, iron deficiency, and magnesium deficiency have all been recognized as factors that could influence overreaching and overtraining [192].
Despite the elevated energy requirements of frequent training [111-114] and increased lean mass, some research indicates that many athletes fail to consume enough calories to maintain energy balance [147]. A survey of elite junior athletes revealed that a high proportion were not in energy balance, failed to meet carbohydrate or micronutrient recommendations, and presented with depleted stores of iron and vitamin D [115].
You may have noticed that when you increase training volume you tend to eat more. Like eating a large pizza after leg day. However, large energy expenditure by athletes does not necessarily induce a compensatory increase in food consumption [66]. Possible reasons for poor intake include; lack of appetite and lack of awareness about the importance of food.
A negative energy balance is a risk factor for overtraining since it can increase fatigue and RPE [1, 8]. Low energy availability have been directly linked to performance in athletes [1]. For instance, one study found athletes in an energy deficit of ~8% for 12 weeks had decreased performance after 6 weeks [116]. In addition to that, long-term caloric restriction can lead to changes in hormonal status and muscle mass especially in physique athletes [117, 118].
If an athlete is going to be in a carbohydrate restricted state they should be aware of creating a negative energy balance, which carries a high risk of maladaptation, infection and overtraining [8]. Basically, if an athlete is going to use a low carbohydrate diet they should be careful with training load/intensity.
Ultimately, overreaching while in a caloric deficit for long periods may lead to UPS.
Below we have some nutritional strategies you can use to improve immune function. This should help, because lowered immunity could lead to UPS.
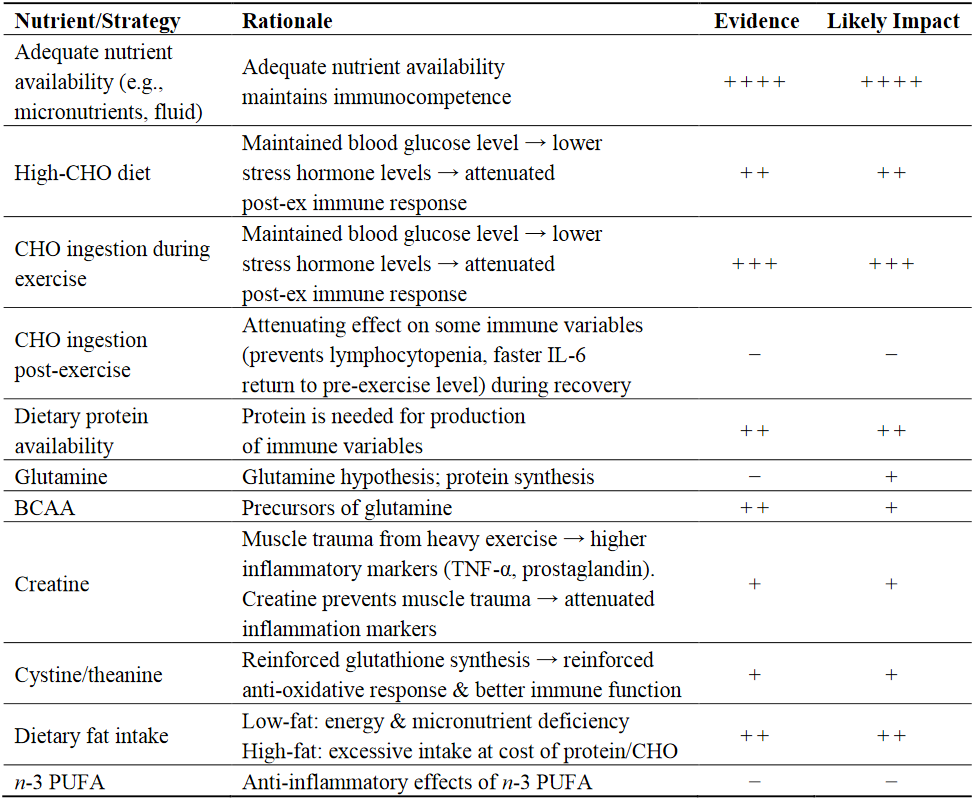
Table by Gunzer et al., 2012
Recovering from overtraining
Mind-body therapies
Mind-body therapies (MBT) like yoga, mindfulness, meditation, and stress-management could speed up the recovery from UPS. In one study, athletes who were diagnosed with overtraining syndrome were assigned to a MBT group, and they compared their overtraining recovery to a control group. The MBT group returned 8-10% faster to their previous training capacity. With that said, their recovery was still incomplete 2 years after they had started the recovery program [11].

Table from (Brooks et al., 2013). SM = Stress Management group.
Sadly, there isn’t a ton of direct studies on how to treat overtraining with MBT, but there are studies on prevention. It’s highly likely that there’s overlap between overtraining prevention and treatment. For example, good mindsets, good social support, and a realistic coach all help prevent overtraining development. Those things don’t suddenly become unimportant once an athlete is underperforming. Now the question is whether changing mindset, improving social support, and getting a better coach speed up the recovery process. Sadly, there’s not enough evidence for us to answer that… Yet.
Go to the prevention section to learn more.
Rest
When prevention fails, rest seems to be the main treatment for UPS, despite the fact that you may become deconditioned during this time [1-4]. The length of rest can vary from six to twelve weeks or more. It can be very difficult to expect highly motivated individuals to simply stop exercising. Some data indicates that low level exercise can benefit recovery [3, 24]. It is still unclear whether complete rest or relative rest is most beneficial, so motivation for exercise should be considered [10, 24]. Treatment with selective serotonin reuptake inhibitor could be beneficial based on the similarities between neuroendocrine changes involved in depression and overtraining [119]. In addition, if sleep disturbance is prominent, treatment with sleep aids could be beneficial [119].
Diagnosing overtraining
Diagnose yourself using this flowchart

Chart by Meeusen et al., 2013
One of the most difficult parts of overtraining is diagnosis. As you can see in the chart above, it is mainly a diagnosis of exclusion because we must systematically rule out other potential things that could make you underperform [26]. Hence, we should exclude certain disease states that share many common qualities with overtraining including; endocrinological disorders (thyroid or adrenal gland, diabetes, vitamin D deficiency), anaemia, or infectious diseases (including viruses, hepatitis, mononucleosis etc.) [10]. Other major disorders such as anorexia, bulimia and depression should also excluded. However, some of these may occur in parallel with UPS, which is why it is so difficult to diagnose. The term “syndrome” emphasizes that training is not the sole causative factor [66].
Underperformance persists despite a period of recovery lasting months or years [10-11, 15]. Importantly, as there is no diagnostic tool to identify an athlete as suffering from overtraining, diagnosis can only be made by excluding all other possible influences on changes in performance and mood state. In other words, if no explanation for the observed changes can be found, overtraining is diagnosed.
Despite decades of research on the syndrome of UPS, early and unequivocal recognition is difficult because the only consistent sign is a decrease in performance with continued training.
The symptoms associated with overtraining vary between individuals, but there is some data to suggest that those in aerobic sports may have changes such as fatigue, depression, resting HR changes and apathy which are typically linked to parasympathetic alterations. In contrast, those in anaerobic sports often have sympathetic changes, such as insomnia, irritability, agitation and increased heart-rate or blood pressure [1, 66, 121].
Why it is difficult to diagnose underperformance
Underperformance Syndrome is notoriously difficult to diagnose because it closely resembles overreaching [1, 32]. Overreaching occurs when we temporarily push beyond our ability to recover [1, 32]. Planned overreaching (aka functional overreaching) is used by athletes, powerlifters, etc. to improve their performance. This type of overreaching is functional because it pushes the body to adapt without pushing it too far [1, 32]. However, this requires a short break or deload after overreaching [1, 32]. The methods vary and are beyond the scope of this article, but there are numerous resources if you need more information.
The illustration below shows the training spectrum.

Illustration from Carfagno and Hendrix, 2014
Though overreaching can be a useful tool, it can be a gateway to something worse. Several authors now think extended overreaching (training hard for a couple of weeks) can turn into Non-functional Overreaching (NFOR) [32]. NFOR is very similar to overtraining in its symptoms which makes it very difficult to distinguish between the two conditions [1, 32]. However, most researchers argue it takes less time to recover from NFOR [32]. It takes more than four weeks of intensified exercise to induce overtraining [13].
Yet, that’s just from the perspective of training. There are now several studies that indicate athletes can get overtraining without increasing their training load [13].
Eventually, if an athlete continues to push him or herself beyond their capacity, they might eventually develop overtraining [1]. Some authors now speculate that overtraining syndrome links with Chronic Fatigue Syndrome (CFS) [11, 13, 18, 187]. A debilitating fatigue disorder that could take years to fully recover from [187]. It’s possible that overreaching, UPS, and CFS exist on a continuum where more stress pushes athletes toward the unsafe side of the spectrum while recovery moves athletes towards “safety” (see illustration below) [1,11, 13, 187].

Illustration partially based on materials from Carfagno and Hendrix, 2014
From an analytical perspective, this continuum makes it very difficult to properly identify whether an athlete is overreaching, underperforming, or chronically fatigued. However, one diagnostic criteria is to see how long it takes the athlete to fully recover (given cessation from training). If it takes a week, it’s probably functional overreaching. Two weeks, it might be NFOR. A month or two, perhaps UPS. A year or two, CFS. The problem is that this diagnosis can only happen after the athlete has fully recovered (retrospectively) [8].
Individual variation and genetic influences
Many studies have tried to diagnose overtraining syndrome in various populations. Not only do they have problems because it is hard to distinguish overtraining from overreaching [1], but also because people experience wildly different symptoms [1, 13, 15, 30, 122]. Some people may become depressed, while others become angry. Some may develop sleep problems, while others lose their sense of hunger and thus lose weight. Furthermore, biomarkers like hormone secretion and heart-rate may vary intra-individually and inter-individually [8, 12, 31, 66,123]. This variation makes diagnosis difficult because few diagnostic criteria apply to everyone [8, 123]. People also have varying training tolerances:
“It is hard to tell if overtraining has occurred because of individual differences in training tolerance. Overtraining for one person may be optimal training for another.”
(Brooks et al., 2013)
It is difficult to determine exactly where the inter-individual variation comes from. Some argue it is genetically predetermined [124]. Recently, several genetic mutations (polymorphisms) have been identified [125, 126]. These polymorphisms could influence training adaptations [127, 128]. There also appears to be an inter-individual differences to endurance or strength training programs [129]. We could even classify individuals as non-, moderate, or extreme responders based on genetics [130-133, 191]. Yet, some disagree since almost everyone adapts in some capacity [134].
These responder phenotypes may not apply directly to studies examining elite athletes because they are presumably hard-working and genetically gifted. However, inter-individual differences could occur because studies lack a high enough population to find a group-type physiological differences even at the elite level. Yet, almost all of the studies are powered properly and can find statistical differences. For example, one method that has come to the forefront of data interpretation is effect size, which is often used in meta-analysis [135-138]. If studies had more homogenous methods, then we could pool them and have a better picture. In the future larger studies with genetic and epigenetic research may shed even more light on the subject of UPS.
Physical factors
Some athletes may recover from a state of overreaching in two weeks [139-141], and this condition is a relatively normal and harmless stage of the training process. If an athlete starts to present more evident problems such as sleep disturbances, loss of weight or appetite, reduced libido, and heavy legs the concern for overtraining should escalate [2, 12].
Injury risk is another critical factor associated with UPS. It’s particularly important to avoid injury and illness because it can lead to worsened long-term athletic performance [142]. This is because program adherence correlates with achieving training goals [142].
One review found overtraining can lead to increased injury risk in elite athletes [16]. Another found that there was a linear relationship between hours of sport play and injury, with athletes who trained more than 16 hours/week having an increased risk of injury. In fact, volume and intensity of training are correlated with overuse injury risk [17]. Though some believe other factors play a bigger role [5]. An acute injury is easily diagnosed, but those related to overuse are much more difficult. Some studies suggest that high absolute loads are not the problem, rather the sharp increase in load compared to normal training [22].
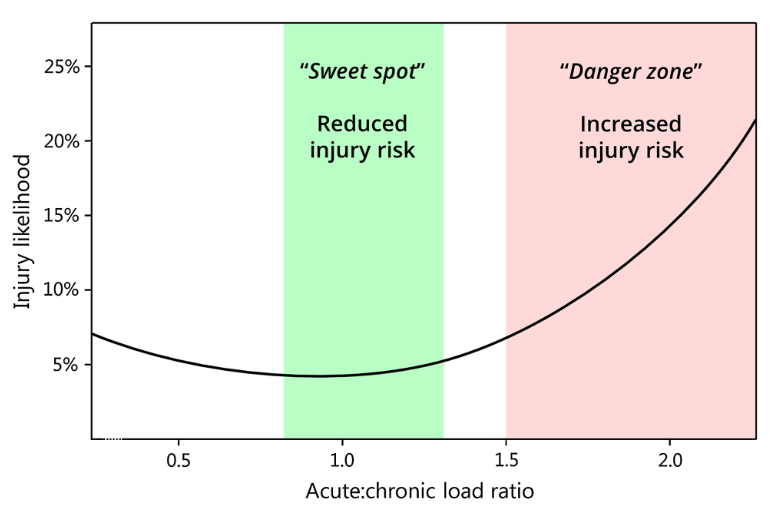
Figure by Soligard et al., 2016
Physiology

Illustration by Fry et al., 1991
There are numerous biomarkers that may identify overtraining which include: inflammatory cytokines, plasma glutamine, creatine kinase activity, blood lactate, and testosterone:cortisol ratio – all of which have differing amounts of data to support them [143].
Among the numerous issues with biomarkers, reliability is a big one. We have to identify changes not only from an athlete’s baseline, but also from OR to truly distinguish when athletes are entering UPS. As you can imagine, the sheer number of studies on biomarkers can be overwhelming, thus we have whittled it down for relevance.
When we think of biomarkers, the most common thought is quantification via blood markers. However, new technology has enabled many biomarkers to be drawn from saliva [123]. Saliva can be taken rapidly, and more important - noninvasively. However, biomarkers in blood are found at a much higher concentration than in saliva [144]. This is important if we have to hit a threshold for detection.
First, let’s identify the major hypothesis within the literature. I’ve honestly never seen so many for one non-disease related problem.
The Cytokine Hypothesis speculates there is a high level of microtrauma to joints, muscle and connective tissue from high volume exercise, which results in local and systemic inflammation. As a result, inflammatory proteins (cytokines, lymphocytes, neutrophils and monocytes) are increased in order to act directly on multiple physiological systems resulting in a disruption of homeostasis. Some of these include IL-6, and TNF-alpha. Glutamine is metabolized at a high rate by immune cells, although it is unclear how changes in plasma glutamine relate to immune status in athletes [13, 145]. An elevated white cell count can even be severe enough to temporarily mimic sepsis [146]. Further confounding these potential markers are changes due to training. For example, neutrophil number may remain elevated for several hours post exercise, but lymphocyte and natural killer cells are depressed [74, 147]. Athletes have normal resting leukocyte counts [148], but endurance athletes can have lower counts [150]. It is likely that small changes in numerous immune markers can synergize to make athletes more susceptible to sickness due to a lower host defense [150].
The HPA Hypothesis notes that prolonged training can cause an autonomic imbalance, resulting in a reduced responsiveness to acetylcholine, which the body then compensates by increasing secretion from the pituitary gland. The idea is the body can compensate in an overreached state until the physiological strain is too much. Ultimately, athletes will cease to compensate with increased ACTH levels and show signs of fatigue [11]. There’s a lot more to this idea, but the data supporting it is scarce.
The Glycogen Depletion Hypothesis supposes that reduced glycogen causes increased oxidation and decreased levels of BCAA which may be involved in fatigue development [10]. If you’ve ever trained while on a long-term caloric deficit you have probably experienced a decrease in performance. Indeed, some studies have found a single bout of short-term exhaustive exercise can reduce glycogen stores ~25-30% [151-158] and low levels of glycogen have been associated with impairments of performance even in short-term exercise [151, 152, 157]. However, some scientists believe there may be another mechanism responsible because if athletes increase their carbohydrate intake they can still suffer from overtraining [106, 159].
Others have proposed that elevated levels of catecholamines may reduce glycogen synthesis after intense exercise [160, 161]. We also know that some cytokines can decrease hunger, which could further reduce glycogen stores [162].
What’s interesting is this hypothesis inherently ties in with the BCAA Hypothesis which is based on the blood-brain barrier. Briefly, serotonin precursor (5-HT) competes with BCAA for the same carrier, but exercise causes increased oxidation of BCAA, which then facilitates increased tryptophan entry into the brain. Yet, if athletes are consuming adequate protein this may not be an issue.
If we take all of these into account rather than look at them on an individual basis, it appears that these responses fit the third stage of the General Adaptation Syndrome [163] and they might be more related to survival than adaptation [13]. Interestingly, energy expenditure can be redirected to immune or HPA function which may further decrease adaptation to training. Often the most difficult interpretation is when these biomarkers are changed, which confounds our ability to determine if one system alone is responsible. It’s a very standard problem in the human body, everything interacts as a system, not an island.
What about the hormone hypothesis?! I can hear the echoes already. Enter, the testosterone:cortisol (T:C) ratio, often used as an indicator of anabolic/catabolic balance. Testosterone’s role in exercise is becoming more controversial – or the idea that it may play a more important role in muscle metabolism during recovery [137, 138] (for review see Tzur 2016) than in muscle growth [164, 165].
Cortisol is perceived as a catabolic hormone, but is known to elevate metabolic rate [166]. Elevated cortisol could translate to long-term consequences affecting body composition or glycogen storage. The T:C ratio decreases in relation to intensity and duration of exercise, as well as during periods of intense training [167]. Only a few studies have shown value in assessing training status through testosterone:cortisol ratio [101, 188-189]. While others have not.
Almost all hormones are under some type of feedback control, some by other hormones, metabolites or other factors. The feedback relationship is the reason why assessment is so difficult. If we look back to the introduction, we must view overtraining as the end of a continuum with the result being a maladaptation of multiple systems [1]. Some of these responses also occur in a chronic energy deficiency with sports, regardless of training status. There are other problems with biomarker data including exercise conditions, nutrition, circadian pulsatility, female hormonal cycles, and stress.
The most challenging factor in recognizing OTS is that it usually develops slowly over months, so if we’re not tracking it frequently we may miss physiological changes.
Psychology

Table by Angeli et al., 2004
The complex nature of emotions
As we've mentioned in the prevention section, there are links between mood and performance. In addition, there are also links between mood <-> immune function [27, 168], and mood <-> hormones [12]. Other factors affect mental health as well, like the microbiome [169, 170, 190]. In addition to these links, there’s evidence that hormones modulate immunity [12] and that mental stress leads to hormonal changes and increased disease risk [171]. Psychological stress is associated with illness [27].
If we look at UPS, many studies and reviews find that certain mood-states can lead to the development of overtraining, and overtraining itself could negatively affect mood-states [1, 2, 12, 32].
This data just underlines how important it is for us to have a macro perspective when analyzing underperformance. Many of the systems we’re looking at are interconnected and a change in one system will probably affect other systems. If we were to speculate, could an unhealthy diet negatively affect the microbiome which would in turn affect mental health which then would increase risk of UPS?
You can look at your mental state to see if you're at risk of underperformance, as per the POMS chart (OTS = overtraining):

Bar chart by Meeusen et al., 2013 (Adapted from Raglin & Morgan, 1994)
Strength training and overtraining
Overtraining syndrome is mainly studied in endurance athletes and these type of athletes accrue much more training volume than people who resistance train. For example, a long distance runner may spend 10+ hours a week actually running, while a resistance-based athlete will only spend a very small amount of time moving weight. Even though this is at a higher magnitude it still gives the body more time to adapt. There are multiple Olympic and National distances in endurance events, yet powerlifting and bodybuilding are not as popular - though they are gaining ground quickly.
There are a few studies that attempt to measure overtraining in resistance exercise. Dr. Fry created a system where subjects would complete ten reps of a 1RM (smith machine) squat every day for two weeks. We know that there is a difference of trained vs untrained, so it’s important to mention these subjects were trained for ~4 yrs and could squat at least 1.5x bodyweight.
Per Meeusen’s guidelines, there was one indication of UPS: Fry caused a decrease in performance. His subjects had a 10-15% drop in 1RM squat after two weeks straight of training at 10 sets of 1 rep at 1RM [143, 144, 172-175]. There are several issues with Fry’s experimental idea of overtraining in strength training:
- Two minute rests between reps
- The weight was dropped 4.5kg on a missed lift
- Unrealistic training method
- The OT group was eating +1100kcal
Different physiological responses occur in aerobic and anaerobic training [180-182]. During the Fry studies and others [15], there is no iceberg profile, or association of POMS with performance. This could make it more difficult to track mental health. However, training session questionnaires did indicate the overtraining group in one study did not look forward to the daily sessions and reported decreased perceptions of strength and recovery. Another study by Fry indicates there was 2-8 week period before members of the OT group could utilize previous levels of training [34]. This means, the subjects in Fry’s studies may not have had overtraining because they returned to normal within ~8 weeks. Based on all of Fry’s work we can sum it up as: intensity-related overtraining does not alter resting hormones associated with decreased performance, but volume-related overtraining does appear to significantly change hormone concentrations.
One of the limitations in resistance training studies is that muscle strength is usually preserved during UPS, but power and sprinting are the first types of performance to decrease. Therefore, athletes may feel sluggish and perform worse, which could lead to a downward spiral of mental and physical health while they continue to try and push through training.
Conclusions
Overtraining deals with the complex interplay between emotions, immunity, neuro-endocrinology, diseases, illnesses, and athletic performance.
The consensus in the scientific literature is that once you’ve developed overtraining, your options are very limited. There is no quick fix to this long-term problem. The optimal solution to overtraining is to prevent it from ever happening.
The body adapts best to small, frequent challenges followed by proper recovery rather than massive challenges all at once. In fact, from our findings in this article, we would say massive challenges is not a good way to progress a training program.
We propose several strategies for preventing overtraining, including properly periodised and individualized training programs, training logs, periodic mental-health self-assessment, avoiding long-term caloric deficits, eating sufficient carbohydrates, having social support, sleep recommendations, meditation/yoga, and using planned and reactive deloads.
References
- Meeusen, R., et al., Prevention, diagnosis, and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med Sci Sports Exerc, 2013. 45(1): p. 186-205.
- Peluso, M.A. and L.H. Guerra de Andrade, Physical activity and mental health: the association between exercise and mood. Clinics (Sao Paulo), 2005. 60(1): p. 61-70.
- Morgan, W.P., et al., Psychological monitoring of overtraining and staleness. Br J Sports Med, 1987. 21(3): p. 107-14.
- Meeusen, R., et al., Diagnosing overtraining in athletes using the two-bout exercise protocol. Br J Sports Med, 2010. 44(9): p. 642-8.
- Winsley, R. and N. Matos, Overtraining and elite young athletes. Med Sport Sci, 2011. 56: p. 97-105.
- Hooper, S.L. and L.T. Mackinnon, Monitoring overtraining in athletes. Recommendations. Sports Med, 1995. 20(5): p. 321-7.
- Verma, S.K., S.R. Mahindroo, and D.K. Kansal, Effect of four weeks of hard physical training on certain physiological and morphological parameters of basket-ball players. J Sports Med Phys Fitness, 1978. 18(4): p. 379-84.
- Lewis, N.A., et al., Can clinicians and scientists explain and prevent unexplained underperformance syndrome in elite athletes: an interdisciplinary perspective and 2016 update. BMJ Open Sport Exerc Med, 2015. 1(1): p. e000063.
- Gould, D., et al., A survey of U.S. Atlanta and Nagano Olympians: variables perceived to influence performance. Res Q Exerc Sport, 2002. 73(2): p. 175-86.
- Kreher, J.B., Diagnosis and prevention of overtraining syndrome: an opinion on education strategies. Open Access J Sports Med, 2016. 7: p. 115-22.
- Brooks K, C.J., McCoy S, The effects of stress management on non-training stress in the overtraining syndrome. International Journal of Physical Medicine & Rehabilitation 2013.
- Fry, R.W., A.R. Morton, and D. Keast, Overtraining in athletes. An update. Sports Med, 1991. 12(1): p. 32-65.
- MacKinnon, L.T., Special feature for the Olympics: effects of exercise on the immune system: overtraining effects on immunity and performance in athletes. Immunol Cell Biol, 2000. 78(5): p. 502-9.
- Hackney, A.C. and K.J. Koltun, The immune system and overtraining in athletes: clinical implications. Acta Clin Croat, 2012. 51(4): p. 633-41.
- Budgett, R., et al., Redefining the overtraining syndrome as the unexplained underperformance syndrome. Br J Sports Med, 2000. 34(1): p. 67-8.
- Rice, S.M., et al., The Mental Health of Elite Athletes: A Narrative Systematic Review. Sports Med, 2016. 46(9): p. 1333-53.
- DiFiori, J.P., et al., Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. Clin J Sport Med, 2014. 24(1): p. 3-20.
- Brown JF, W.M., Sharp CS, “Down but Not out”: An Exploration of the Psychological Factors That Impact the Unexplained Underperformance Syndrome (UPS). International Journal of Sports Science & Coaching, 2006.
- Cunha GS, R.J., Oliveria AR, Overtraining: theories, diagnosis and markers. Revista Brasileira de Medicina do Esporte, 2006. 12(5).
- Lastella, M., et al., Sleep/wake behaviours of elite athletes from individual and team sports. Eur J Sport Sci, 2015. 15(2): p. 94-100.
- Clement, D.B., J.E. Taunton, and G.W. Smart, Achilles tendinitis and peritendinitis: etiology and treatment. Am J Sports Med, 1984. 12(3): p. 179-84.
- Soligard, T., et al., How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med, 2016. 50(17): p. 1030-41.
- Soligard, T., M. Schwellnus, and J.M. Alonso, Infographic. International Olympic Committee consensus statement on load in sport and risk of injury: how much is too much? Br J Sports Med, 2016. 50(17): p. 1042.
- Budgett, R., Fatigue and underperformance in athletes: the overtraining syndrome. Br J Sports Med, 1998. 32(2): p. 107-10.
- Budgett, R., et al., The effects of the 5-HT2C agonist m-chlorophenylpiperazine on elite athletes with unexplained underperformance syndrome (overtraining). Br J Sports Med, 2010. 44(4): p. 280-3.
- Teeple, E., R.M. Shalvoy, and E.R. Feller, Overtraining in young athletes. Med Health R I, 2006. 89(7): p. 236-8.
- Schwellnus, M., et al., How much is too much? (Part 2) International Olympic Committee consensus statement on load in sport and risk of illness. Br J Sports Med, 2016. 50(17): p. 1043-52.
- Bartholomew, J.B., et al., Strength gains after resistance training: the effect of stressful, negative life events. J Strength Cond Res, 2008. 22(4): p. 1215-21.
- Ruuska, P.S., et al., Self-rated mental stress and exercise training response in healthy subjects. Front Physiol, 2012. 3: p. 51.
- Kenttä, G., P. Hassmen, and J.S. Raglin, Training practices and overtraining syndrome in Swedish age-group athletes. Int J Sports Med, 2001. 22(6): p. 460-5.
- Snyder, A.C., The Endocrine System in Overtraining. Endocrinology of Physical Activity and Sports, 2013: p. 523-584.
- Winsley, R.J., G.L. Battersby, and H.C. Cockle, Heart rate variability assessment of overreaching in active and sedentary females. Int J Sports Med, 2005. 26(9): p. 768-73.
- Veale, D.M., Psychological aspects of staleness and dependence on exercise. Int J Sports Med, 1991. 12 Suppl 1: p. S19-22.
- Fry, R.W., et al., Psychological and immunological correlates of acute overtraining. Br J Sports Med, 1994. 28(4): p. 241-6.
- Meeusen, R., et al., Brain neurotransmitters in fatigue and overtraining. Appl Physiol Nutr Metab, 2007. 32(5): p. 857-64.
- Hill, A.P. and P.R. Appleton, The predictive ability of the frequency of perfectionistic cognitions, self-oriented perfectionism, and socially prescribed perfectionism in relation to symptoms of burnout in youth rugby players. J Sports Sci, 2011. 29(7): p. 695-703.
- Hill, A.P., H.K. Hall, and P.R. Appleton, Perfectionism and athlete burnout in junior elite athletes: the mediating role of coping tendencies. Anxiety Stress Coping, 2010. 23(4): p. 415-30.
- Lemyre, P.N., H.K. Hall, and G.C. Roberts, A social cognitive approach to burnout in elite athletes. Scand J Med Sci Sports, 2008. 18(2): p. 221-34.
- Gustafsson H, H.P., Kentta G, Johansson M, A qualitative analysis of burnout in elite Swedish athletes. Psychology of Sport and Exercise, 2008. November
- Ho MS, A.P., Cumming J, Duda JL. , Examining the Relationship Between Perfectionism Dimensions and Burning Out Symptoms in Deaf and Hearing Athletes. Journal of Clinical Sport Psychology, 2015(June).
- Jowett GE, H.A., Howard HK, Curran T, Perfectionism, burnout and engagement in youth sport: The mediating role of basic psychological needs. Psychology of Sport and Experience, 2016. 24.
- Raglin, J.S., W.P. Morgan, and P.J. O'Connor, Changes in mood states during training in female and male college swimmers. Int J Sports Med, 1991. 12(6): p. 585-9.
- Stults-Kolehmainen, M.A. and J.B. Bartholomew, Psychological stress impairs short-term muscular recovery from resistance exercise. Med Sci Sports Exerc, 2012. 44(11): p. 2220-7.
- Stults-Kolehmainen, M.A.,R. Sinha, The effects of stress on physical activity and exercise. Sports Med, 2014. 28(7): p. 2007-17.
- Morgan, N., et al., The effects of mind-body therapies on the immune system: meta-analysis. PLoS One, 2014. 9(7): p. e100903.
- Huynh, J.Y., D. Xanthopoulou, and A.H. Winefield, Social support moderates the impact of demands on burnout and organizational connectedness: a two-wave study of volunteer firefighters. J Occup Health Psychol, 2013. 18(1): p. 9-15.
- JH, Lu et al., Interaction of athletes' resilience and coaches' social support on the stress-burnout relationship: A conjunctive moderation perspective. . Psychology of Sport and Exercise, 2016.
- Amaranath, B., H.R. Nagendra, and S. Deshpande, Effect of integrated Yoga module on positive and negative emotions in Home Guards in Bengaluru: A wait list randomized control trial. Int J Yoga, 2016. 9(1): p. 35-43.
- Angeli, A., et al., The overtraining syndrome in athletes: a stress-related disorder. J Endocrinol Invest, 2004. 27(6): p. 603-12.
- Demarzo, M.M., et al., The Efficacy of Mindfulness-Based Interventions in Primary Care: A Meta-Analytic Review. Ann Fam Med, 2015. 13(6): p. 573-82.
- Dharmawardene, M., et al., A systematic review and meta-analysis of meditative interventions for informal caregivers and health professionals. BMJ Support Palliat Care, 2016. 6(2): p. 160-9.
- Goyal, M., et al., Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Intern Med, 2014. 174(3): p. 357-68.
- Kim, S.M., J.M. Park, and H.J. Seo, Effects of mindfulness-based stress reduction for adults with sleep disturbance: a protocol for an update of a systematic review and meta-analysis. Syst Rev, 2016. 5: p. 51.
- Pascoe, M.C. and I.E. Bauer, A systematic review of randomised control trials on the effects of yoga on stress measures and mood. J Psychiatr Res, 2015. 68: p. 270-82.
- Niles, H., et al., Functional genomics in the study of mind-body therapies. Ochsner J, 2014. 14(4): p. 681-95.
- Solberg, E.E., et al., Meditation: a modulator of the immune response to physical stress? A brief report. Br J Sports Med, 1995. 29(4): p. 255-7.
- Solberg, E.E., et al., Stress reactivity to and recovery from a standardised exercise bout: a study of 31 runners practising relaxation techniques. Br J Sports Med, 2000. 34(4): p. 268-72.
- Wahbeh, H., et al., Mind-Body Medicine and Immune System Outcomes: A Systematic Review. Open Complement Med J, 2009. 1: p. 25-34.
- Nagendra, R.P., N. Maruthai, and B.M. Kutty, Meditation and its regulatory role on sleep. Front Neurol, 2012. 3: p. 54.
- Neuendorf, R., et al., The Effects of Mind-Body Interventions on Sleep Quality: A Systematic Review. Evid Based Complement Alternat Med, 2015. 2015: p. 902708.
- Ong, J.C., et al., A randomized controlled trial of mindfulness meditation for chronic insomnia. Sleep, 2014. 37(9): p. 1553-63.
- Bower, J.E. and M.R. Irwin, Mind-body therapies and control of inflammatory biology: A descriptive review. Brain Behav Immun, 2016. 51: p. 1-11.
- Moen F, F.R., Abrahamsen FE, Examining possible relationships between mindfulness, stress, school - and sport performance and athlete burnout. . International Journal of Coaching Science, 2015.
- Isoard-Gautheur, S., et al., Associations between the perceived quality of the coach-athlete relationship and athlete burnout: An examination of the mediating goal of achievement goals . Psych Sport Ex, 2016. 37(4): p. 436-48.
- Kreher, J.B. and J.B. Schwartz, Overtraining syndrome: a practical guide. Sports Health, 2012. 4(2): p. 128-38.
- Purvis, D., S. Gonsalves, and P.A. Deuster, Physiological and psychological fatigue in extreme conditions: overtraining and elite athletes. PM R, 2010. 2(5): p. 442-50.
- Hutton, J., D. Wellington, and S. Miller, Exercise-induced rhabdomyolysis. N Z Med J, 2016. 129(1442): p. 89-92.
- Knapik, J.J., Extreme Conditioning Programs: Potential Benefits and Potential Risks. J Spec Oper Med, 2015. 15(3): p. 108-13.
- Knapik, J.J. and F.G. O'Connor, Exertional Rhabdomyolysis: Epidemiology, Diagnosis, Treatment, and Prevention. J Spec Oper Med, 2016. 16(3): p. 65-71.
- Lee, G., Exercise-induced rhabdomyolysis. R I Med J (2013), 2014. 97(11): p. 22-4.
- Lin, H., W. Chie, and H. Lien, Epidemiological analysis of factors influencing an episode of exertional rhabdomyolysis in high school students. Am J Sports Med, 2006. 34(3): p. 481-6.
- Keah, S. and K. Chng, Exercise-Induced Rhabdomyolysis with Acute Renal Failure After Strenuous Push-UPS. Malays Fam Physician, 2009. 4(1): p. 37-9.
- Sandhu, R.S., et al., Renal failure and exercise-induced rhabdomyolysis in patients taking performance-enhancing compounds. J Trauma, 2002. 53(4): p. 761-3; discussion 763-4.
- Nieman, D.C., Current perspective on exercise immunology. Curr Sports Med Rep, 2003. 2(5): p. 239-42.
- Bamji, Z.D. and G.E. Haddad, Convergence of theories of alcohol administration postanabolic stimulation on mTOR signaling: lessons for exercise regimen. Alcohol Clin Exp Res, 2015. 39(5): p. 787-9.
- Barnes, M.J., Alcohol: impact on sports performance and recovery in male athletes. Sports Med, 2014. 44(7): p. 909-19.
- Parr, E.B., et al., Alcohol ingestion impairs maximal post-exercise rates of myofibrillar protein synthesis following a single bout of concurrent training. PLoS One, 2014. 9(2): p. e88384.
- Thomas, D.T., K.A. Erdman, and L.M. Burke, Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J Acad Nutr Diet, 2016. 116(3): p. 501-28.
- Pyne, D.B. and M. Gleeson, Effects of intensive exercise training on immunity in athletes. Int J Sports Med, 1998. 19 Suppl 3: p. S183-91; discussion S191-4.
- van Dijk, J.G. and K.D. Matson, Ecological Immunology through the Lens of Exercise Immunology: New Perspective on the Links between Physical Activity and Immune Function and Disease Susceptibility in Wild Animals. Integr Comp Biol, 2016. 56(2): p. 290-303.
- Gleeson, M. and D.B. Pyne, Respiratory inflammation and infections in high-performance athletes. Immunol Cell Biol, 2016. 94(2): p. 124-31.
- Robson-Ansley, P.J., M. Gleeson, and L. Ansley, Fatigue management in the preparation of Olympic athletes. J Sports Sci, 2009. 27(13): p. 1409-20.
- Bryant, P.A., J. Trinder, and N. Curtis, Sick and tired: Does sleep have a vital role in the immune system? Nat Rev Immunol, 2004. 4(6): p. 457-67.
- Banks, S. and D.F. Dinges, Behavioral and physiological consequences of sleep restriction. J Clin Sleep Med, 2007. 3(5): p. 519-28.
- Watson, N.F., et al., Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep, 2015. 38(6): p. 843-4.
- Strand B, F.A., The Impact of Sleep on Youth Athletic Performance. 2015.
- Dashti, H.S., et al., Short sleep duration and dietary intake: epidemiologic evidence, mechanisms, and health implications. Adv Nutr, 2015. 6(6): p. 648-59.
- Nedelec, M., et al., Stress, Sleep and Recovery in Elite Soccer: A Critical Review of the Literature. Sports Med, 2015. 45(10): p. 1387-400.
- Sargent, C., et al., The impact of training schedules on the sleep and fatigue of elite athletes. Chronobiol Int, 2014. 31(10): p. 1160-8.
- Sargent, C., et al., The validity of activity monitors for measuring sleep in elite athletes. J Sci Med Sport, 2016. 19(10): p. 848-53.
- Yarnell, A.M. and P. Deuster, Sleep As A Strategy For Optimizing Performance. J Spec Oper Med, 2016. 16(1): p. 81-5.
- P, Bird., Sleep, Recovery, and Athletic Performance: A Brief Review and Recommendations. Strength and Conditioning Journal, 2013.
- Fullagar, H.H., et al., Sleep and athletic performance: the effects of sleep loss on exercise performance, and physiological and cognitive responses to exercise. Sports Med, 2014. 45(2): p. 161-86.
- Thun, E., et al., Sleep, circadian rhythms, and athletic performance. Sleep Med Rev, 2014. 23: p. 1-9.
- Hawley JA, L.B., Carbohydrate availabiliity and training adaptation: effects on cell metabolism. Exercse Sports Science Reviews, 2010(Octoer).
- Kingsbury, K.J., L. Kay, and M. Hjelm, Contrasting plasma free amino acid patterns in elite athletes: association with fatigue and infection. Br J Sports Med, 1998. 32(1): p. 25-32; discussion 32-3.
- Witard, O.C., et al., Effect of increased dietary protein on tolerance to intensified training. Med Sci Sports Exerc, 2011. 43(4): p. 598-607.
- Hansen, M., et al., Protein intake during training sessions has no effect on performance and recovery during a strenuous training camp for elite cyclists. J Int Soc Sports Nutr, 2016. 13: p. 9.
- Kraemer, W.J., et al., The effects of amino acid supplementation on hormonal responses to resistance training overreaching. Metabolism, 2006. 55(3): p. 282-91.
- Halson, S.L., Sleep in elite athletes and nutritional interventions to enhance sleep. Sports Med, 2014. 44 Suppl 1: p. S13-23.
- Halson, S.L. and A.E. Jeukendrup, Does overtraining exist? An analysis of overreaching and overtraining research. Sports Med, 2004. 34(14): p. 967-81.
- Kirwan, J.P., et al., Physiological responses to successive days of intense training in competitive swimmers. Med Sci Sports Exerc, 1988. 20(3): p. 255-9.
- Kirwan, J.P., et al., Carbohydrate balance in competitive runners during successive days of intense training. J Appl Physiol (1985), 1988. 65(6): p. 2601-6.
- Kirwan, J.P., D. O'Gorman, and W.J. Evans, A moderate glycemic meal before endurance exercise can enhance performance. J Appl Physiol (1985), 1998. 84(1): p. 53-9.
- Costill, D.L., Carbohydrates for exercise: dietary demands for optimal performance. Int J Sports Med, 1988. 9(1): p. 1-18.
- Snyder, A.C., et al., Overtraining following intensified training with normal muscle glycogen. Med Sci Sports Exerc, 1995. 27(7): p. 1063-70.
- Robson, P., Elucidating the unexplained underperformance syndrome in endurance athletes : the interleukin-6 hypothesis. Sports Med, 2003. 33(10): p. 771-81.
- Aragon, A.A. and B.J. Schoenfeld, Nutrient timing revisited: is there a post-exercise anabolic window? J Int Soc Sports Nutr, 2013. 10(1): p. 5.
- Burke, L.M., L.J. van Loon, and J.A. Hawley, Post-exercise muscle glycogen resynthesis in humans. J Appl Physiol (1985), 2016: p. jap 00860 2016.
- Kerksick, C., et al., International Society of Sports Nutrition position stand: nutrient timing. J Int Soc Sports Nutr, 2008. 5: p. 17.
- Aniceto RR, R.-D.R., Scott CB, Lima MF, , Acute effects of different weight training methods on energy expenditure in trained men. EXERCISE AND SPORTS MEDICINE CLINIC, 2013.
- Haddock BL, W.L., Resistance training volume and post exercise energy expenditure. Int J Sports Med, 2006.
- Reis MV, S.C., Modeling the Total Energy Costs of Resistance Exercise: a Work in Progress. Central European Journal of Sport Sciences and Medicine, 2016. 14(November ).
- Scala D, M.J., Rozenek R, Stone M, Metabolic Cost of a Preparatory Phase of Training in Weight Lifting: A Practical Observation. Journal of Strength & Conditioning Research, 1987.
- Garcia-Roves, P.M., et al., Nutrient intake and food habits of soccer players: analyzing the correlates of eating practice. Nutrients, 2014. 6(7): p. 2697-717.
- Vanheest, J.L., et al., Ovarian suppression impairs sport performance in junior elite female swimmers. Med Sci Sports Exerc, 2014. 46(1): p. 156-66.
- Helms, E.R., A.A. Aragon, and P.J. Fitschen, Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. J Int Soc Sports Nutr, 2014. 11: p. 20.
- Trexler, E., et al.,Metabolic adaptations for weight loss: implications for the athlete. JISSN, 2014. 11(14): p. 1038-42.
- Pearce, P.Z., A practical approach to the overtraining syndrome. Curr Sports Med Rep, 2002. 1(3): p. 179-83.
- Budgett, R., ABC of sports medicine. The overtraining syndrome. BMJ, 1994. 309(6952): p. 465-8.
- Lehmann, M., et al., Autonomic imbalance hypothesis and overtraining syndrome. Med Sci Sports Exerc, 1998. 30(7): p. 1140-5.
- Platen, P., Overtraining and the Endocrine System - Part 1 Terminology European Journal of Sport Science, 2010. 1(February).
- Papacosta, E. and G.P. Nassis, Saliva as a tool for monitoring steroid, peptide and immune markers in sport and exercise science. J Sci Med Sport, 2011. 14(5): p. 424-34.
- Bouchard, D.R., M. Heroux, and I. Janssen, Association between muscle mass, leg strength, and fat mass with physical function in older adults: influence of age and sex. J Aging Health, 2011. 23(2): p. 313-28.
- Roth, S.M., Genetic aspects of skeletal muscle strength and mass with relevance to sarcopenia. Bonekey Rep, 2012. 1: p. 58.
- Tan, L.J., et al., Molecular genetic studies of gene identification for sarcopenia. Hum Genet, 2012. 131(1): p. 1-31.
- Thomis, M.A., et al., Exploration of myostatin polymorphisms and the angiotensin-converting enzyme insertion/deletion genotype in responses of human muscle to strength training. Eur J Appl Physiol, 2004. 92(3): p. 267-74.
- Timmons, J.A., Variability in training-induced skeletal muscle adaptation. J Appl Physiol (1985), 2011. 110(3): p. 846-53.
- Bamman, M.M., et al., Cluster analysis tests the importance of myogenic gene expression during myofiber hypertrophy in humans. J Appl Physiol (1985), 2007. 102(6): p. 2232-9.
- Thalacker-Mercer, A., et al., Cluster analysis reveals differential transcript profiles associated with resistance training-induced human skeletal muscle hypertrophy. Physiol Genomics, 2013. 45(12): p. 499-507.
- Thalacker-Mercer, A.E., J.K. Petrella, and M.M. Bamman, Does habitual dietary intake influence myofiber hypertrophy in response to resistance training? A cluster analysis. Appl Physiol Nutr Metab, 2009. 34(4): p. 632-9.
- Davidsen, P.K., et al., High responders to resistance exercise training demonstrate differential regulation of skeletal muscle microRNA expression. J Appl Physiol (1985), 2011. 110(2): p. 309-17.
- Stec, M.J., et al., Ribosome biogenesis may augment resistance training-induced myofiber hypertrophy and is required for myotube growth in vitro. Am J Physiol Endocrinol Metab, 2016: p. ajpendo 00486 2015.
- Churchward-Venne, T.A., et al., There Are No Nonresponders to Resistance-Type Exercise Training in Older Men and Women. J Am Med Dir Assoc, 2015. 16(5): p. 400-11.
- Schoenfeld, B.J., D. Ogborn, and J.W. Krieger, Dose-response relationship between weekly resistance training volume and increases in muscle mass: A systematic review and meta-analysis. J Sports Sci, 2016: p. 1-10.
- Schoenfeld, B.J., D. Ogborn, and J.W. Krieger, Effects of Resistance Training Frequency on Measures of Muscle Hypertrophy: A Systematic Review and Meta-Analysis. Sports Med, 2016. 46(11): p. 1689-1697.
- Schoenfeld, B.J., D.I. Ogborn, and J.W. Krieger, Effect of repetition duration during resistance training on muscle hypertrophy: a systematic review and meta-analysis. Sports Med, 2015. 45(4): p. 577-85.
- Schoenfeld, B.J., et al., Muscular adaptations in low- versus high-load resistance training: A meta-analysis. Eur J Sport Sci, 2016. 16(1): p. 1-10.
- Jeukendrup, A.E. and M.K. Hesselink, Overtraining--what do lactate curves tell us? Br J Sports Med, 1994. 28(4): p. 239-40.
- Kreider, R.B., et al., Effects of creatine supplementation on body composition, strength, and sprint performance. Med Sci Sports Exerc, 1998. 30(1): p. 73-82.
- Steinacker, J.M., et al., Training of junior rowers before world championships. Effects on performance, mood state and selected hormonal and metabolic responses. J Sports Med Phys Fitness, 2000. 40(4): p. 327-35.
- Raysmith, B.P. and M.K. Drew, Performance success or failure is influenced by weeks lost to injury and illness in elite Australian track and field athletes: A 5-year prospective study. J Sci Med Sport, 2016. 19(10): p. 778-83.
- Fry, A.C., W.J. Kraemer, and L.T. Ramsey, Pituitary-adrenal-gonadal responses to high-intensity resistance exercise overtraining. J Appl Physiol (1985), 1998. 85(6): p. 2352-9.
- Gleeson, M., The scientific basis of practical strategies to maintain immunocompetence in elite athletes. Exerc Immunol Rev, 2000. 6: p. 75-101.
- Mackinnon, L.T. and S. Hooper, Mucosal (secretory) immune system responses to exercise of varying intensity and during overtraining. Int J Sports Med, 1994. 15 Suppl 3: p. S179-83.
- Ostrowski, M.A., et al., Expression of chemokine receptors CXCR4 and CCR5 in HIV-1-infected and uninfected individuals. J Immunol, 1998. 161(6): p. 3195-201.
- Nieman, D.C., Exercise immunology: future directions for research related to athletes, nutrition, and the elderly. Int J Sports Med, 2000. 21 Suppl 1: p. S61-8.
- Gleeson, M. and N.C. Bishop, The T cell and NK cell immune response to exercise. Ann Transplant, 2005. 10(4): p. 43-8.
- Degerstrom, J. and B. Osterud, Increased inflammatory response of blood cells to repeated bout of endurance exercise. Med Sci Sports Exerc, 2006. 38(7): p. 1297-303.
- Mackinnon, L.T., Immunity in athletes. Int J Sports Med, 1997. 18 Suppl 1: p. S62-8.
- Balsom, P.D., et al., High-intensity exercise and muscle glycogen availability in humans. Acta Physiol Scand, 1999. 165(4): p. 337-45.
- Balsom, P.D., et al., Carbohydrate intake and multiple sprint sports: with special reference to football (soccer). Int J Sports Med, 1999. 20(1): p. 48-52.
- Bangsbo, J., et al., Muscle lactate metabolism in recovery from intense exhaustive exercise: impact of light exercise. J Appl Physiol (1985), 1994. 77(4): p. 1890-5.
- Bangsbo, J., et al., Elevated muscle glycogen and anaerobic energy production during exhaustive exercise in man. J Physiol, 1992. 451: p. 205-27.
- Bangsbo, J. and F. Lindquist, Comparison of various exercise tests with endurance performance during soccer in professional players. Int J Sports Med, 1992. 13(2): p. 125-32.
- Bangsbo, J., L. Norregaard, and F. Thorsoe, The effect of carbohydrate diet on intermittent exercise performance. Int J Sports Med, 1992. 13(2): p. 152-7.
- Skein, M., et al., The effects of carbohydrate intake and muscle glycogen content on self-paced intermittent-sprint exercise despite no knowledge of carbohydrate manipulation. Eur J Appl Physiol, 2012. 112(8): p. 2859-70.
- Essen, B., Glycogen depletion of different fibre types in human skeletal muscle during intermittent and continuous exercise. Acta Physiol Scand, 1978. 103(4): p. 446-55.
- Snyder, A.C., Overtraining and glycogen depletion hypothesis. Med Sci Sports Exerc, 1998. 30(7): p. 1146-50.
- Armstrong, L.E., Nutritional strategies for football: counteracting heat, cold, high altitude, and jet lag. J Sports Sci, 2006. 24(7): p. 723-40.
- Delp, M.D. and R.B. Armstrong, Is glycogen depletion related to muscular activity? J Appl Physiol (1985), 1988. 65(1): p. 490-1.
- Carfagno, D.G. and J.C. Hendrix, 3rd, Overtraining syndrome in the athlete: current clinical practice. Curr Sports Med Rep, 2014. 13(1): p. 45-51.
- Selye, H., The general-adaptation-syndrome. Annu Rev Med, 1951. 2: p. 327-42.
- Damas, F., et al., Resistance training-induced changes in integrated myofibrillar protein synthesis are related to hypertrophy only after attenuation of muscle damage. J Physiol, 2016. 594(18): p. 5209-22.
- Mitchell, W.K., et al., Human Skeletal Muscle Protein Metabolism Responses to Amino Acid Nutrition. Adv Nutr, 2016. 7(4): p. 828S-38S.
- Brillon, D.J., et al., Effect of cortisol on energy expenditure and amino acid metabolism in humans. Am J Physiol, 1995. 268(3 Pt 1): p. E501-13.
- Urhausen, A., H. Gabriel, and W. Kindermann, Blood hormones as markers of training stress and overtraining. Sports Med, 1995. 20(4): p. 251-76.
- Pariante, CM . Neuroscience, mental health and the immune system: overcoming the brain-mind-body trichotomy. Epidemiology and Psychiatric Sciences 2016.
- Kennedy PJ, M.A., Cryan JF, Stanton C., Microbiome in Brain Function and Mental Health. Trends in Food Science & Technology, 2016.
- Sandhu KV, S.E., Cryan JC, Feeding the microbiota-gut-brain axis: diet, microbiome, and neuropsychiatry. The Journal of Laboratory and Clinical Medicine, 2016.
- Ranabir, S. and K. Reetu, Stress and hormones. Indian J Endocrinol Metab, 2011. 15(1): p. 18-22.
- Fry, A.C. and W.J. Kraemer, Resistance exercise overtraining and overreaching. Neuroendocrine responses. Sports Med, 1997. 23(2): p. 106-29.
- Fry, A.C., et al., Performance decrements with high-intensity resistance exercise overtraining. Med Sci Sports Exerc, 1994. 26(9): p. 1165-73.
- Fry, A.C., et al., beta2-Adrenergic receptor downregulation and performance decrements during high-intensity resistance exercise overtraining. J Appl Physiol (1985), 2006. 101(6): p. 1664-72.
- Fry, R.W., A.R. Morton, and D. Keast, Periodisation and the prevention of overtraining. Can J Sport Sci, 1992. 17(3): p. 241-8.
- Maughan, Overreaching and Unexplained Underperformance Syndrome: Nutritional Interventions. The Encyclopaedia of Sports Medicine: An IOC Medical Publication. Vol. 19. 2013.
- Budgett R, N.E., Lehmann C, Sharp C, Jones D, Peto T, Collins D, Neurkar R, White P, Redefining the overtraining syndrome as the unexplained underperformance syndrome. British Journal of Sports Medicine, 2000. 34(1).
- Lin AC, L.C., Wang TL, Leu JG, Rhabdomyolysis in 119 students after repetitive exercise. British Journal of Sports Medicine, 2005(January).
- Fardal H, G.L., [Exercise-induced rhabdomyolysis - a new trend?]. Tidsskr Nor Laegeforen., 2016.
- Hakkinen K, P.A., Alen M, Kauhanen H, Komi PV, Neuromuscular and hormonal adaptations in athletes to strength training in two years. J Appl Physiology, 1988. December (6).
- Van Borselen F, V.N., Kraemer WJ, Exercise Physiology Corner: the role of anaerobic exercise in overtraining. Strength and Conditioning Journal, 1992.
- Brown JF, W.M., Sharp CS, “Down but Not out”: An Exploration of the Psychological Factors That Impact the Unexplained Underperformance Syndrome (UPS). International Journal of Sports Science & Coaching, 2006.
- Roy, B., Overreaching/Overtraining: More is Not Always Better. ACSM'S Health & Fitness Journal, 2015. 19(2).
- Bryan S and Pinto G. The Effect of Mindfulness Meditation Techniques During Yoga and Cycling. Alternative and Complementary Therapies, 2014. 20(December).
- Appleton, H., Hill, Relations between multidimensional perfectionism and burnout in junior-elite male athletes. Psychology of Sport and Exercise 2009. 10(4): p. 457-465.
- Ivy and Ferguson-Stegall,Nutrient Timing: The Means to Improved Exercise Performance, Recovery, and Training Adaptation. American Journal of Lifestyle Medicine, 2013.
- Brown, M.A., AB; Jason LA, Illness Duration and Coping Style in Chronic Fatigue Syndrome. Psychology Repository, 2011.
- Urhausen, A., H. Gabriel, and W. Kindermann, Blood hormones as markers of training stress and overtraining. Sports Med, 1995. 20(4): p. 251-76.
- Duclos, M., C. Gouarne, and D. Bonnemaison, Acute and chronic effects of exercise on tissue sensitivity to glucocorticoids. J Appl Physiol (1985), 2003. 94(3): p. 869-75.
- Clara Seira Oriacha, R.C.R., , Catherine Stantonc, d, John F. Cryand, e, Timothy G. Dinan, Food for thought: The role of nutrition in the microbiota-gut–brain axis. Clinical Nutrition Experimental, 2016. 6(April): p. 25-38.
- McGlory, C. and S.M. Phillips, Exercise and the Regulation of Skeletal Muscle Hypertrophy. Prog Mol Biol Transl Sci, 2015. 135: p. 153-73.
- Maffetone, P.B. and P.B. Laursen, Athletes: Fit but Unhealthy? Sports Med Open, 2015. 2: p. 24.