![]()
![]()

Plain Language Summary
Ketosis, simplified
The ketogenic diet
The ketogenic diet is a type of very-low carbohydrate diet. The goal of the diet is to get you into ketosis, usually by eating less than 50 grams of carbs per day (Adam-Perrot et al., 2006; Westman et al., 2007; Accurso et al., 2008; Bueno et al., 2013; Paoli et al., 2013; Gregory et al., 2017).
Yet, the 50 g carb “limit” might vary from person to person (Adam-Perrot et al., 2006). Hence, we can’t say that 50 g is a rule that applies to everyone. In fact, data indicate that the carb limit is higher. We will cover this in-depth in part 3 of this series. Subscribe to the newsletter to stay informed.
In terms of dietary protein and fat, the keto diet isn’t set in stone. It is usually moderate/high protein and high fat, but there are several variants of the ketogenic diet. The classic variant sometimes used to manage epilepsy is very high fat, low carb, and low protein (Roehl and Sewak, 2017).
Ketosis
Ketosis takes place when your body lacks carbohydrates as a primary fuel source (Adam-Perrot et al., 2006; Westman et al., 2007). It is a natural response to starvation, extended fasting, and prolonged exercise (Mitchell et al., 1995; Laffel, 1999; VanItallie and Nufert, 2003; Cox and Clarke, 2014; Newman and Verdin, 2017; Puchalska and Crawford, 2017). Note that ketosis takes place because carbs are limited, not because fat intake is high.
“Ketogenesis is an evolutionary adaptation conserved within all higher order organisms to sustain survival during famine, illness or energetic stress” - Cox and Clarke, 2014
During ketosis, the metabolism shifts towards primarily using fat and ketones (Laffel, 1999; Adam-Perrot et al., 2006; Westman et al., 2007; Paoli et al., 2013; Paoli, 2014). The body is generally very adaptive, and can use whichever fuel is available (Helge et al., 2001; Coyle et al., 2001; Spriet and Watt, 2003; Gregory et al., 2011; Spriet et al., 2014; Loher et al., 2016). This is called substrate utilization, and is usually discussed in relation to exercise intensity (example: Coyle et al., 1995). Some research suggests that ketone bodies can be glucose sparing (Laffel, 1999; Newman and Verdin, 2017).
“The term ketone bodies (KB) refers to three metabolites: acetoacetate [AA], β-hydroxybutyrate [BHB], and acetone.” -Westman et al., 2003
To figure out when someone is in ketosis, we can measure ketone levels in blood, urine, or breath (Laffel, 1999; Clocker et al., 2013; Anderson, 2015; Urbain and Bertz, 2016). The urinary measurement is somewhat inconsistent because it varies drastically throughout the day and night (Urbain and Bertz, 2016). Some suggest that blood measurements are superior (Clocker et al., 2013; Urbain and Bertz, 2016; Brooke et al., 2016).
With a ketogenic diet, it should take a couple of days to enter ketosis (Langfort et al., 1997; Willi et al., 1998; Harber et al., 2005; Klement et al., 2013; Urbain et al., 2017). Still, this does not imply that the body is completely fat-adapted in such a short time period 1This topic will be covered in-depth in later parts of the series. Physiological adaptations as well as changes in glycogen and body water take place over a longer period.

Figure by Harber et al., 2005 shows that ketone levels of BHB significantly increased in a manner of days. Subjects ate 5% carbs (absolute values not reported).
Will a high protein intake prevent ketosis?
It has been said that eating a lot of protein will kick you out of ketosis because of gluconeogenesis 2When protein is turned into glucose. In spite of this claim, protein intakes from 122 to 176 grams (1.1-2.2 g/kg) per day did not prevent ketosis in several studies.
Studies reporting protein and ketone levels

Ketosis vs. ketoacidosis
Lastly, we need to distinguish between physiological ketosis and the harmful ketoacidosis (Laffel, 1999). The former is a normal state as described above, while ketoacidosis is a state of chronic, severe ketosis that primarily affects type 1 diabetics (Laffel, 1999; Puchalska and Crawford, 2017). The complication occurs when there is a lack of insulin and levels of ketones plus other hormones become excessively high (Laffel, 1999; Perilli et al., 2013; Oliver, 2015; Tran et al., 2017). Ketones are acidic and can be buffered when they’re below certain levels (Oliver, 2015). Elevated levels can result in acidosis (blood becomes too acidic) (Oliver, 2015). If left untreated, ketoacidosis can be very harmful and even deadly (Tran et al., 2017).
Ketoacidosis can also happen during starvation or when drinking excessive amounts of alcohol (McGuire et al., 2006; Sinha et al., 2014; Mostert and Bonavia, 2016; Noor et al., 2016)
Basics of weight gain and loss
The scientific consensus is that calories in vs. calories out (CICO) determines weight loss and weight gain.
Eating in an energy surplus leads to body weight gain. We see this effect in both metabolic ward studies (Bray et al., 2012; Apolzan et al., 2014; Bray et al., 2015), and in less controlled settings (Norgan and Durnin, 1980; Lammert et al., 2000; Sato et al., 2014; Anderson et al., 2017)
A caloric deficit typically causes us to lose weight, but if we eat sufficient amounts of protein and do strength training, we can retain or increase muscle mass. This is why it’s very important to distinguish between weight loss and fat loss. Weight loss includes loss of fat mass and lean mass (i.e. water, glycogen, and muscle protein).
Challenging this model, some keto proponents argue that it is the degree of ketosis or insulin inhibition that leads to fat loss. According to this argument, the decrease in insulin and elevation in ketones is what leads the body to become fat adapted. The body should then burn more body fat compared to a calorie restricted diet. As such, keto may have a “metabolic advantage” (Volek et al., 2004).
To answer whether keto is superior for burning fat, we’ve compared both the CICO model and carb restriction model in the sections below.
How keto affects body fat and muscle mass
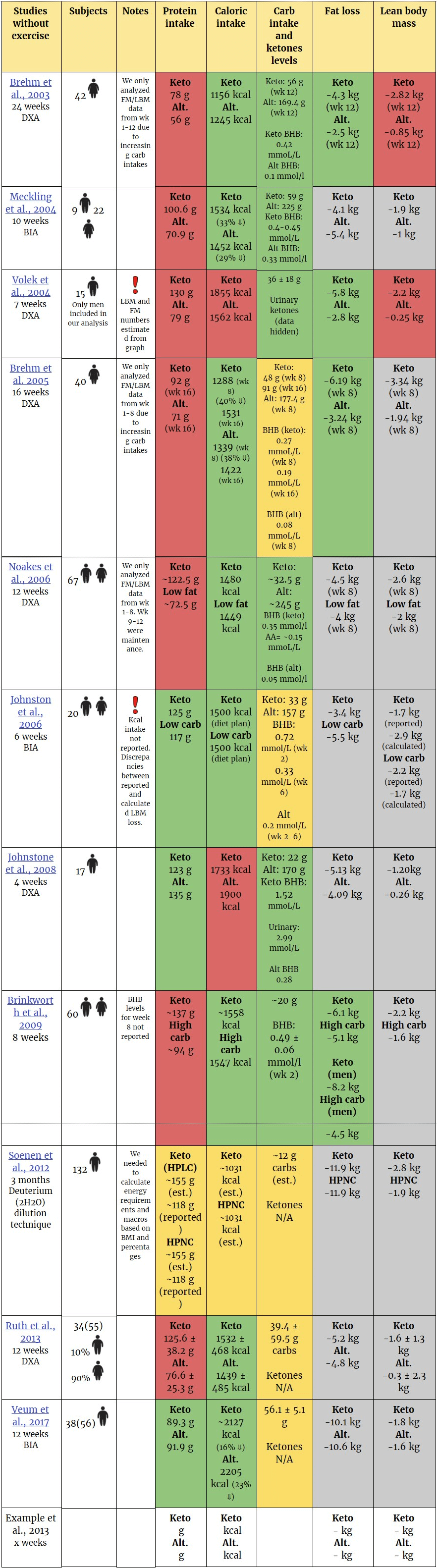
Overview of the literature
In this section, we’ve summarized the keto research on humans. Overall, the data follows predictable patterns. A caloric deficit lead to loss of fat and lean body mass, however lean mass was typically retained or increased when subjects did strength training and ate enough protein.
 Beware of interpreting these numbers without context.
Beware of interpreting these numbers without context.






Discussing how fat loss compared between groups
Three studies found that keto lost more fat mass than control when calories were matched. In all three of the studies, the participants were obese, and in two studies the participants were women (Brehm et al studies). It’s difficult to say exactly why the keto groups lost more fat, but here are some potential reasons:
- Protein was not matched between groups. Since protein is a satiating macronutrient, it can help adherence to the diet. As such, lower protein intakes may lead people to eat more.
- The Brehm studies asked keto participants to eat ad-libitum (as much food as desired). There may have been a positive psychological effect for this; it is easier to adhere when you don’t have to count calories because you only have to reduce carbs. The control groups, in comparison, had to count calories to hit a specific caloric goal. This could lead to underreporting.
- There might be metabolic advantage to keto.
- Carbohydrate depletion could affect how body fat levels are estimated in most tools that assess body fat (will be discussed in-depth in part 3).
In other studies, control groups lost more fat than the keto groups, but the results weren’t statistically significant (Meckling et al., 2004; Johnston et al., 2006). It’s possible these studies were statistically underpowered to detect differences.
Ketone levels and fat loss
Posed with the uncertainty above, we wanted to further investigate how fat loss is affected by ketosis. In particular, does higher ketone levels lead to greater fat loss?
The graph below shows how much fat keto groups lost in studies where ketone levels were reported. The ketone levels shown are from the last week of the study, average ketone levels, or the ketone level that occurred most commonly during the study. Total fat mass lost was divided by the duration of the study (number of weeks), allowing us to directly compare weekly losses in different studies.

The figure shows ketone levels above and fat loss below the vertical baseline. Both urinary ketones (AA) and blood ketones (BHB) are displayed. |
Correlation between ketones (BHB) and weekly fat loss
When all relevant study groups were included in the analysis (15), BHB levels correlated moderately with weekly fat loss (Pearson’s R = -0.48, R^2 = 0.23).
Note: The red line shown in the regression model is the R^2 line.
Y-axis: weekly fat loss
X-axis: BHB levels (mmol/l)
Each dot represents a study group (keto or control) where BHB levels and fat loss were reported

However, the correlation disappeared (Pearson’s R = 0.06, R^2 = 0.00) after a clear outlier (Q1 – 1.5 × IQR or Q3 + 1.5 × IQR) was removed (the keto group in Johnstone et al., 2008) . The strength and direction of the correlation seems to rely purely on the inclusion/exclusion of this group.

As a side note, these correlations serve as an example of how one could easily “torture” data (tactical exclusions and inclusions) to make it admit to anything.
Limitations of our correlations
- We've run correlations between study averages and we don’t have access to individual data points. Averaged data points aren’t as accurate as individual data.
- Self-reported carb intake isn’t necessarily accurate. The regression analysis relies on accurate data to produce accurate correlations.
- Not enough data: we need more studies
Correlations reported in keto studies
- “Increases in beta-hydroxybutyrate also correlated with the amount of weight loss (Pearson’s r = –0.62, p = 0.0062).” - Meckling et al., 2002
- "... there was no correlation between the level of plasma β-hydroxybutyrate and weight loss (r = 0.29; P = 0.43)." - Brehm et al., 2003
Keto and athletic performance
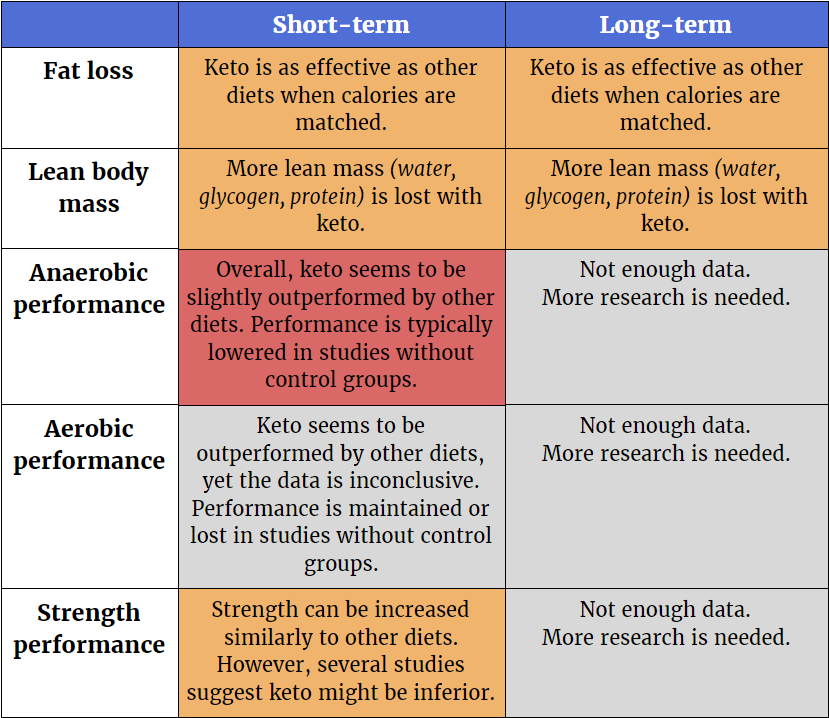
Overview of the literature
Here is a summary table of the performance literature:

How keto affects endurance performance


Discussing endurance performance
Early keto studies suggest that a ketogenic diet can maintain or improve performance (Phinney et al., 1980, Phinney et al., 1983, reviewed in Phinney, 2004) in an overweight and untrained population (Phinney et al., 1980) and in endurance athletes (Phinney et al., 1983). However, these two studies had many limitations, such as the lack of a control group and small number of subjects. In fact, there are several keto studies that lack comparative control groups (Klement et al., 2013, Zinn et al., 2017, Davis and Phinney, 1999, Urbain et al., 2017).
It is also important to remember that a small experimental group could mean one person affects the overall mean (to be covered in future limitations article).

Figure by Brad Dieter and Adam Tzur, based on data from Phinney et al., 1983 were subjects maintained performance on average, yet that is not the case when looking at individual data.
It was later shown in a crossover study that two weeks of ketogenic dieting, compared to two weeks of high-carbohydrate dieting, benefited prolonged submaximal exercise (60% VO2max) without affecting high-intensity endurance performance (90% VO2max) in cyclists. However, nutrition and training data was not provided, which makes it difficult to know exactly what the participants were eating or doing (Lambert et al., 1994).
One study looked at maximal and mean power output after only three days of a ketogenic diet in untrained subjects. There was a significant decrease in mean power and a trending decrease in maximal power output which is likely due to a decrease in glycogen (Langfort et al., 1997).
In 2013, Klement et al., published a pilot case study on the impact of a self-prescribed ketogenic diet (Klement et al., 2013). Five weeks of a ketogenic diet did not impair running performance, but large inter-individual differences existed. Importantly, there was no significant difference in Vo2 max. There was no control group or training data in this study(see above).
In a well-designed study, Burke and colleagues followed race-walkers for 3 weeks over one or two competitions (Burke et al., 2017). They compared high CHO to a ketogenic diet while the athletes were in a slight caloric deficit. The main findings were a) all groups improved performance compared to baseline and b) those on a ketogenic diet failed to improve their 10km performance during the second competition. However, their exercise economy decrease.
In one of the longest ketogenic diet studies to date, Zinn et al, used aged endurance athletes (Zinn et al., 2017). They found a decrease in performance using several tests such as time to exhaustion, Vo2 max, and peak power.
The keto endurance studies are a mixed bag. Many of them have very small sample sizes and are relatively short in duration. Since there seems to be a keto adaptation period, subjects are expected to underperform after a week or two on the diet (Phinney et al., 1980). The results might give us the wrong impression that keto leads to underperforming, even though things might be different if the studies were longer.
Most studies did not control training. They either asked subjects to maintain their regular training program or do no training. This is good for ecological validity. In other words, it tells us how the diet plays out in practice when we don’t control the variables of a person’s life.
For example, if people naturally exercise less when on a keto diet because of fatigue or weakness, then a drop in physical performance would probably follow. But if the participants were “forced” to exercise during the study, then they might improve their performance. However, when people in real life decide to go on a ketogenic diet, they won’t have scientists, doctors, and personal trainers watching over them. So the first scenario is more realistic. The second scenario is necessary when trying to figure out how keto affects people who train.
Lastly, there are many ways to measure aerobic and anaerobic performance (average power, peak power, time to exhaustion, race performance, speed in timed trials, VO2max, etc.). We must remember that one test isn’t necessarily enough to make conclusions about overall “endurance performance”. The term itself is somewhat vague and depends on the sport or activity in question.
In summary, most of the studies suggest that measures of aerobic and anaerobic short-term performance are either decreased or maintained with a ketogenic diet.
How keto affects strength

Note: when calculating averages, the highest numbers were used when ranges were given.


Discussing the keto strength literature
In a study using eight elite gymnasts over 30 days, Paoli et al., found no strength differences in squat jump, countermovement jump, chin-ups, or dips when comparing those on a western diet vs ketogenic diet. There was a small non-significant trend for those on a western diet in pushups (+7) and a small non-significant trend in the leg closed barrier test (+2) for subjects on a keto diet. A major limitation of the study is protein wasn’t matched during the diets and there was no training data.
Another study was completed in a group of taekwondo athletes using a ketogenic diet vs control (Rhyu and Cho, 2014). Rhyu and colleagues found no difference in grip strength.
CrossFit contains a form of resistance training and one keto trial was run for 6 weeks in trained subjects (Gregory et al., 2017). Interestingly, after 6 weeks there was no difference in long jump or vertical jump between keto and control group. All subjects in the study improved total CrossFit performance time and overall power. A few limitations for this study include lack of sufficient ketone measurements, food reporting, and the keto group eating 200 less calories + 10 grams more protein per day.
Lastly, a RCT in untrained older men (age = 59) compared a low-fat diet vs a ketogenic diet, with or without exercise, over the course of 12 weeks (Wood et al., 2012). Comparing across groups that trained, the low fat diet group increased chest press strength twice as much as the keto group. There was also a difference favoring the low-fat diet in leg press (+26%). In contrast, a study by Merielles et al., found no difference in strength measurements when comparing a keto group to a control group (Meirelles and Gomes, 2016).
There are few resistance training studies that use a ketogenic diet. Most of the studies find that both the keto group and the control group can increase their strength.
One problem is that the keto groups eat more protein than the control group in most of the keto studies (Paoli et al., 2012, Rhyu and Cho, 2014, Brinkworth et al., 2009, Wood et al., 2012; Gregory et al., 2017). Further, ketones aren’t always measured, so it’s hard to say for sure that the participants were in ketosis. The one study where protein and calories were matched and ketosis measured, (Wilson et al., 2017) has its own issues.
Overall, we need more protein and calorie-matched studies that also measure ketone bodies. With these limitations noted, keto groups did maintain or increase their strength in the studies. Though, typically not to the same extent as the control group. This is promising because it suggests that a ketogenic diet doesn’t have to entail a loss of strength, but it also implies that people looking to maximize their strength should be careful about choosing keto.
Individual diet responses
Most of our data here deals with how people respond to a diet, on average. However, some studies have also reported the level of success for every individual.
Below you see figures from different studies. Every dot, circle, X, or line represents an individual. You can see that some individuals lost very little weight, while some lost a lot.
Whenever a mean is reported, these individual data points are not included. However, standard deviations (a measure of spread) can be reported alongside the mean to help give us an idea how much variation there is in individual responses.
 Wide variability in absolute weight loss. Figure from Noakes et al., 2006
Wide variability in absolute weight loss. Figure from Noakes et al., 2006
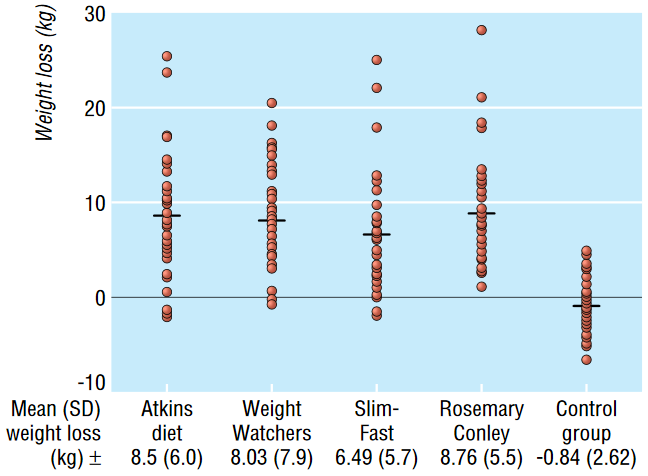 Figure by Truby et al., 2006
Figure by Truby et al., 2006

Figure by Jabekk et al., 2010
Issues in keto research
The keto literature has many issues, conflicts of interest, and limitations.
Here are some examples:
- Many studies measure blood ketone levels, yet several do not. In the latter studies, we do not know if the participants were in a ketogenic state or not.
- Several studies do not directly track how much the study participants ate (i.e. they rely on self-reported food questionnaires). This can be somewhat of a limitation, especially in studies where they didn't measure ketone levels. 4While dietary recalls or food-frequency questionnaires aren't perfect, they are necessary when subjects aren't constantly being monitored (such as in a metabolic ward or hospital setting)
- Keto groups tend to eat more protein and less calories than control groups.
- Many studies have poor methodology or experimental design. 5Many studies also have solid methodologies. The limitations presented here do not imply that the entire keto literature should be rejected, as some have suggested.
- (lack of) carbohydrates affect body composition estimations.
Methodology
Important control questions for every keto study
- Did they do strength training?
- Was the protein intake sufficiently high to maintain lean mass?
- What was the extent of caloric restriction? Greater restriction could lead to greater loss of FM and FFM
- How many daily carbs did the keto group consume?
- Did they measure ketones (urinary/blood)?
- How was FM and FFM measured/estimated?
- Do changes in FM and FFM match changes in body weight?
Inclusion criteria
To be included in our single-arm tables, studies had to:
- Have a dietary intervention where the keto group ate less than ~50 grams of carbs per day
- Include body composition measurements of fat mass (FM) and fat-free mass (FFM)
Exclusion criteria
General exclusion criteria:
- All animal studies
- Studies with major methodological issues
- Studies that do not measure FM/FFM
- Studies that lack of data reporting, to the point where estimating changes in body comp would involve a lot of guesswork and assumptions (i.e. data only presented as percentages, or in low-resolution figures, making estimations difficult)
Our conflicts of interest
This article was written and published without sponsorship from any company, individual, or organization. This website, SCI-FIT, receives no compensation or funding from any source, and is not affiliated with any other companies or organizations.
- Adam Tzur is the head of SCI-FIT. No COIs to report.
- Brandon Roberts works at the University of Alabama at Birmingham. He is also employed by The Strength Guys. No COIs to report.
- Alex Leaf works for Examine.com. No COIs to report.